Impact of Sacubitril/Valsartan on Renal Outcomes in HFpEF Patients



Introduction
Chronic kidney disease (CKD), a common comorbidity in heart failure (HF) patients is associated with a higher risk of cardiovascular (CV) events than in patients without CKD. Renin-angiotensin system (RAS) inhibition reduces mortality in patients with HF with reduced ejection fraction (HFrEF), and retards the progression of proteinuric CKD in patients with diabetes. The evidence on RAS inhibition alone, in patients with HF and preserved ejection fraction (HFpEF) has been inconclusive till date. Addition of neprilysin inhibition along with RAS inhibition has shown renal benefits in HFrEF patients. Similarly in a phase II trial, sacubitril/valsartan has shown renal benefits over valsartan alone in HFpEF patients.
Aim
To assess the renal effects of angiotensin/neprilysin inhibition (Sacubitril/valsartan) in patients with HFpEF
Patient Profile
- Patients with chronic HFpEF (age ≥ 50 years) with New York Heart Association (NYHA) functional classes II to IV, and left ventricular ejection fraction (LVEF) ≥45%
- All patients were on diuretic therapy, had evidence of structural heart disease, along with elevated levels of plasma B-type natriuretic peptide (BNP) or N-terminal pro-B-type natriuretic peptide (NTproBNP).
Methods
Study Design
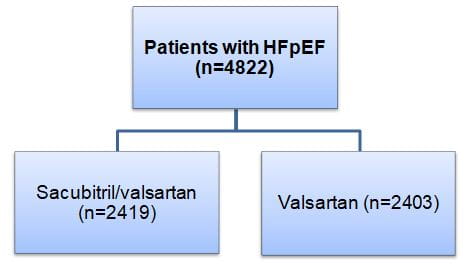
- Post hoc analysis of the “Prospective Comparison of ARNI With ARB Global Outcomes in HF With Preserved Ejection Fraction” (PARAGON-HF)
- PARAGON-HF was a randomized, double-blind, event-driven trial
Treatment Strategy
Outcomes
- Pre-specified renal composite outcome [time to first occurrence of either: ≥50% reduction in estimated glomerular filtration rate (eGFR), end-stage renal disease (ESRD), or death from renal causes]
- The individual components of the composite outcome
- The influence of therapy on eGFR slope
Results
- At randomization, mean eGFR for the study population was 63 ml/min/1.73m2. Based on the baseline eGFR, patients were categorized into two groups as; eGFR<60 and ≥ 60 ml/min/1.73 m2.
- There was a significant 50% reduction in the incidence of composite renal outcome the sacubitril/valsartan vs. valsartan alone group [1.4% vs. 2.7%; hazard ratio (HR); 0.50, 95% confidence interval (CI) 0.33-0.77; P=0.001) (Figure 1)
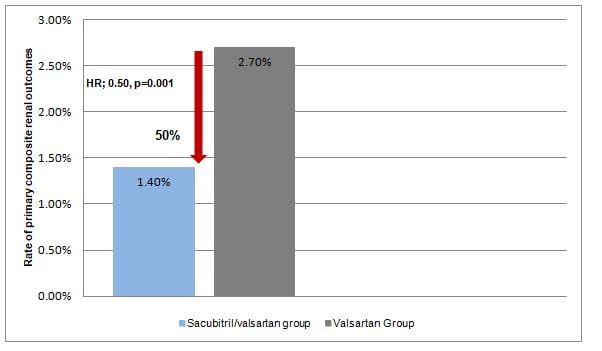
- The 4-year risk of experiencing the renal composite outcome was also lower in sacubitril/valsartan vs. valsartan group (2.1% vs. 4.1%).
- The incidence of composite renal outcomes did not differ significantly as per the baseline eGFR (pinteraction=0.92).
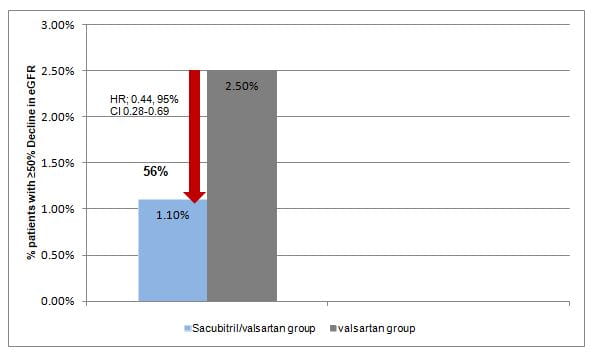
- The results of renal composite outcomes were primarily driven by the individual component of ≥50% reduction in eGFR. There was a significant 56% risk reduction for ≥50% reduction in eGFR in sacubitril/valsartan group vs. valsartan group (Figure 2).
- Fewer patients in the sacubitril/valsartan group vs. valsartan group developed ESRD (0.3% vs. 0.5%, HR; 0.58, 95% CI 0.23-1.47)
- Two deaths due to renal disease were recorded during the study, one in each group
- Mean decline in eGFR during the study was lesser in sacubitril/valsartan group vs. valsartan group [-2.0 (95%CI -2.2 to -1.9) ml/min/1.73 m2 /year vs. -2.7 (95%CI -2.8 to -2.5) ml/min/1.73 m2/year]. Treatment effect estimates remained similar after adjusting for blood pressure during the study
Conclusions
- Amongst patients with HFpEF, sacubitril/valsartan vs. valsartan alone reduced the risk of renal events, and attenuated the decline in eGFR, irrespective of changes in blood pressure.
- The clinical benefits of sacubitril/valsartan in HFpEF patients appeared to be similar across baseline kidney function.
- Sacubitril/valsartan may represent a promising therapeutic option to attenuate the decline in kidney function decline in patients with HFpEF.
Circulation. Aug 17, 2020 (Published Ahead of Print); DOI: 0.1161/CIRCULATIONAHA.120.047643.