CANVAS Program: Impact of Canagliflozin on Cardiovascular and Renal Outcomes in Type-2 Diabetes Patients



Background
Type-2 diabetes mellitus (T2DM) patients are burdened with a substantial risk of cardiovascular (CV) and renal disease. Canagliflozin, a sodium–glucose co-transporter-2 (SGLT2) inhibitor reduces glycemia along with a reduction in blood pressure and body weight in type 2 diabetes patients. Canagliflozin also has a favorable impact on intra-renal hemodynamics and albuminuria.
Aim
The CANVAS (The Canagliflozin Cardiovascular Assessment Study) Program (an integrated analysis of CANVAS and CANVAS-Renal [CANVAS-R] studies) aimed at evaluating the impact of canagliflozin treatment on CV, renal, and safety outcomes in T2DM patients at high risk for cardiovascular disease.
Patient Profile
- Adults with T2DM (glycated hemoglobin [HbA1c]; ≥7% to ≤10.5%) and at high risk of cardiovascular disease (CVD)
- Patients aged ≥30 years with a history of symptomatic CVD or those aged ≥50 years with at least two of the following CVD risk factors:
- Duration of diabetes ≥10 years
- Systolic blood pressure (SBP) >140 mm Hg while receiving ≥1 antihypertensive agents
- Current smoking
- Microalbuminuria or macroalbuminuria,
- High-density lipoprotein-cholesterol (HDL-C) level <38.7 mg/dL (1 mmol/L)
- Baseline estimated glomerular filtration rate (eGFR) >30 ml/min/1.73 m2 of body surface area.
Methods
Study Design
- Randomized double-blind study with a 2-week placebo run-in phase
Treatment Strategy
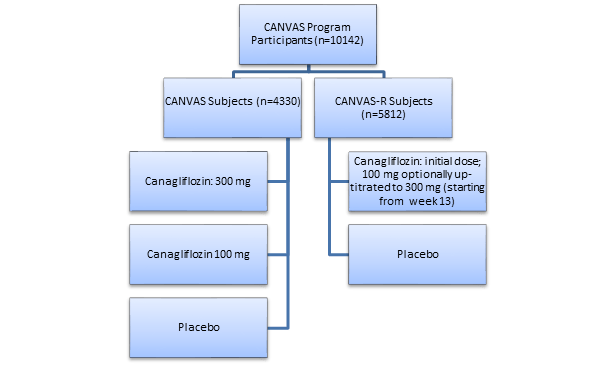
- Participants from CANVAS study were randomized in 1:1:1 ratio and those from the CANVAS-R in 1:1 ratio to receive canagliflozin or placebo
Follow-Up
- CANVAS Program - mean follow-up: 188.2 weeks
- CANVAS – mean follow up: 295.9 weeks
- CANVAS-R – mean follow up: 108 weeks
Outcomes
Primary Outcome
- A composite of death from CV causes, nonfatal myocardial infarction (MI), or nonfatal stroke
Secondary Outcomes
- Death from any cause
- Death from CV causes
- Progression of albuminuria (defined as: a >30% increase in albuminuria and a change from either normoalbuminuria to microalbuminuria/ macroalbuminuria or from microalbuminuria to macroalbuminuria
- The composite of death from CV causes and hospitalization for heart failure
Exploratory Outcomes
Prespecified Cardiovascular Outcomes
- Nonfatal MI
- Nonfatal stroke and
- Hospitalization for heart failure
Prespecified Renal Outcomes
- Regression of albuminuria, and the renal composite comprising a 40% reduction in eGFR sustained for at least two consecutive measures, the need for renal-replacement therapy (dialysis or transplantation), or death from renal causes
Safety Analysis
- Any adverse events
Results
- A total of 96% (n=9734) individuals completed the trial. The mean age of the study subjects was 63.3 years and 35.8% were women. The mean duration of diabetes was 13.5 years, and 65.6% subjects had a history of cardiovascular disease CVD at baseline.
- The incidence of primary outcome was significantly lower in the canagliflozin group vs. the placebo group; a 14% risk reduction in the primary outcome was observed with canagliflozin vs placebo (P<0.001 for noninferiority, P=0.0158 for superiority (Table1)
- The reductions in incidence of fatal secondary outcome including death from any cause, and death from CV causes was statistically non-significant in both the study groups
- Canagliflozin demonstrated a 33% significant reduction in hospitalization due to heart failure as well as a 22% reduction in a composite outcome of CV death or hospitalization due to heart failure
- A 27% reduction in progression of albuminuria and a 70% increase in regression of albuminuria was observed with canagliflozin-treated patients vs. the placebo-treated patients.
- The incidence of renal composite outcome comprising of sustained 40% reduction in eGFR, the need for renal-replacement therapy, or death from renal causes was less frequent in the canagliflozin group vs. the placebo group; a 40% reduction was observed with canagliflozin vs. placebo for this composite outcome (Table 1)
|
Outcome |
Annualized incidence (participants per 1000 patient-years) |
Hazard Ratio (HR) with 95% confidence interval |
Risk Reduction (RR) | |
|
Canagliflozin group |
Placebo group | |||
|
Primary Outcome* |
26.9 |
31.5 |
0.86 (0.75 – 0.97) |
14% |
|
Hospitalization due to heart failure |
5.5 |
8.7 |
0.67 (0.52 – 0.87) |
33% |
|
CV Death or hospitalization due to heart failure |
16.3 |
20.8 |
0.78 (0.67 – 0.91) |
22% |
|
Renal composite outcome^ |
5.5 |
9.0 |
0.60 (0.47 – 0.77) |
40% |
|
*Composite of CV death, nonfatal MI or nonfatal stroke; ^Composite of 40% reduction in eGFR, renal replacement therapy, or renal death | ||||
- Dose of canagliflozin was increased to 300 mg in 71.4% of CANVAS-R participants. All study subjects were treated appropriately with other medications for glycemic control and CV risk.
- The use of other antidiabetic medications during follow-up was 9.3% lower in the group treated with canagliflozin vs. group receiving placebo.
- Over the entire follow-up period, canagliflozin demonstrated greater HbA1c (-0.58%), body weight (-1.6 kg) and SBP (-3.93 mm Hg) reductions compared to placebo (P<0.001 for all comparisons)
- Canagliflozin-treated patients had an increase in HDL-C (2.05 mg/dL) as well as LDL-C (4.68 mg/dL) vs. placebo group. However, the LDL-C to HDL-C ratio remained unchanged
- The incidence of serious adverse events was less frequent in the canagliflozin group vs. placebo group (104.3 vs. 120.0 participants with an event per 1000 patient-years; HR 0.93)
- A higher risk of amputation, although of very low incidence (6.3 vs. 3.4 participants with amputation per 1000 patient-years; HR 1.97) was observed with canagliflozin compared to placebo. Majority of the amputations (71%) occurred at the level of the toe or metatarsal. The highest absolute risk of amputation was observed in patients with a history of amputation or peripheral arterial disease, but relative risk with canagliflozin vs. placebo was similar across these subgroups.
- Canagliflozin did not increase the risk of hypoglycemia, hyperkalemia, acute kidney injury, pancreatitis, malignancies, or venous thromboembolism vs. placebo
- The incidence of all fractures was higher in the canagliflozin group vs. the placebo group (15.4 vs. 11.9 participants with fracture per 1000 patient-years; HR 1.26). A similar trend was observed for low-trauma fractures events as well (11.6 vs. 9.2 participants with fracture per 1000 patient-years; HR 1.23 non-significant). Further, low-trauma fracture incidence was higher in canagliflozin group vs. placebo in CANVAS but not in CANVAS-R.
- The incidence of ketoacidosis was less frequent in both, canagliflozin and placebo groups (0.6 vs. 0.3 participants with an event per 1000 patient years; HR 2.23)
Conclusions
- When added to the current standard of care, canagliflozin further lowered the risk of CV events in T2DM patients at high risk of CVD
- Canagliflozin also demonstrated reduction in renal outcomes
- Canagliflozin treatment was associated with a higher risk of amputation, although of very low incidence, compared to current standard of care
N Engl J Med. 2017; 377: 644 - 57