Pulmonary Rehabilitation - An Insight



Recent Updates in Chronic Obstructive Pulmonary Disease1
As per the World Health Organization (WHO) 2015 estimates, 65 million people worldwide have moderate to severe chronic obstructive pulmonary disease (COPD). Globally by 2030, COPD is projected to become the third leading cause of death. In COPD patients, healthcare professionals (HCPs) play an important role in improving health-related quality of life (HRQoL) and health-related outcomes. Updated Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations 2015 suggests both pharmacological and non-pharmacological strategies in management of stable COPD.
Management of COPD
Pharmacological Therapy
- For patients with few symptoms and a low-risk of exacerbations: A short-acting bronchodilator is the first-line recommendation.
- For all other patients: Long-acting β2-agonists (LABAs), for example, formoterol, olodaterol, indacaterol and vilanterol or long-acting antimuscarinics (LAMAs), for example, tiotropium, glycopyrronium, umeclidinium or aclidinium, alone or in LABA/LAMA combinations, are recommended.
- For patients at high-risk of exacerbations: Inhaled corticosteroids (ICS) are combined with LABAs or LAMAs, for example, budesonide + formoterol, fluticasone + salmeterol, fluticasone + vilanterol and mometasone + formoterol.
- For COPD patients with forced expiratory volume 1 (FEV1) < 50% predicted, chronic bronchitis and frequent exacerbations: Phosphodiesterase-4 (PDE-4) inhibitor, roflumilast.
Non-pharmacological Therapy
Pulmonary rehabilitation (PR) is recommended for all symptomatic COPD patients, regardless of severity and involves exercise training, patient education, nutritional advice and psychosocial support.
- Short-term oxygen therapy is suggested for patients hospitalized with an exacerbation.
- Long-term oxygen therapy is suggested for patients who remain hypoxemic at discharge/with chronic respiratory failure, with non-invasive ventilation in those with stable, very severe COPD.
Importance of Physical Activity and Exercise
Irrespective of grades of COPD, regular physical activity helps:
- Symptom control
- Reduces rates of hospitalization, improves morbidity
- Improves all-cause mortality and respiratory mortality
Exercise training (alone or as part of a PR program) has been shown to improve dyspnea, fatigue, exercise intolerance, exercise capacity, muscle weakness and HRQoL and reduce hospitalization frequency.
Advantages of Pulmorehab on COPD Patients2
COPD: A Systemic Disease with Effort Limitation
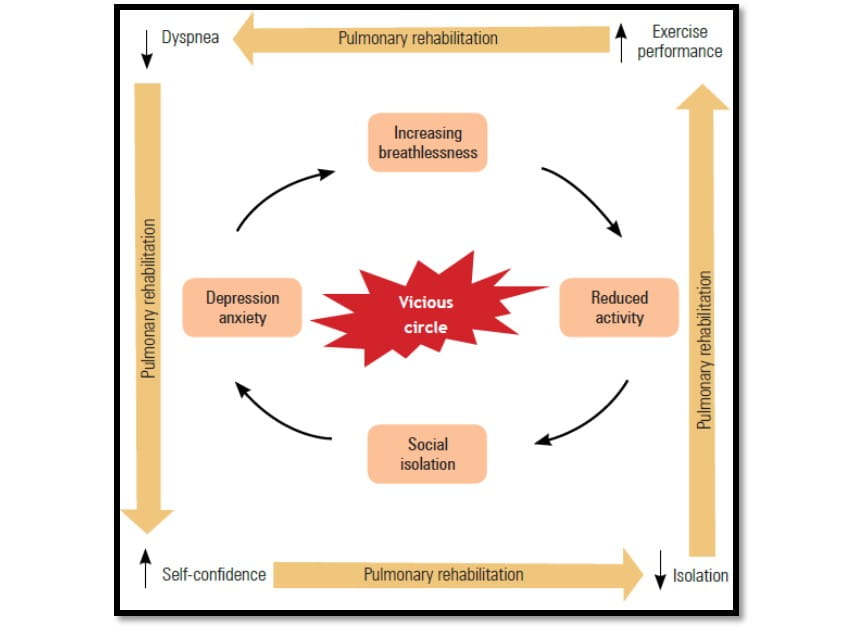
For many years, COPD was considered to be a respiratory disease, mainly caused by tobacco smoking and leading to progressive dyspnea. This increases the need of PR in COPD patients (Figure 1).
PR
The updated statement by the American Thoracic Society and the European Respiratory Society (ATS/ERS) Task Force on PR gives the following definition of PR:
PR is a comprehensive intervention based on a thorough patient assessment followed by patient-tailored therapies, which include, but are not limited to, exercise training, education and behavior change, designed to improve the physical and emotional condition of people with chronic respiratory disease and to promote the long-term adherence of health-enhancing behaviors. Thereby using a holistic approach, PR aims to reverse the systemic manifestations of COPD as well as to relieve the fears and anxiety associated with social and exterior activities, thus leading to a change in the patient’s day-to-day life. Finally, it aims to break the aforementioned vicious circle in COPD.
Who Should Attend a PR Program?
All the patients suffering from a chronic respiratory disease of whatever origin, who have a decrease of pulmonary function, who are symptomatic and who have intolerance to effort, in spite of an optimal pharmacological treatment.
Evidence of the Effectiveness of PR in COPD
Many published randomized controlled trials (RCTs), renowned committees, guidelines and meta-analysis have demonstrated the effectiveness and utility of PR on symptomatic COPD patients. The main outcomes, including exercise performance, dyspnea, HRQoL, psychosocial benefits, cost effectiveness, reduced health care utilization and survival (Table 1) have been reported.
|
Outcome |
Source |
Comments |
|
Improvement of exercise performance |
ACCP/AACVPR |
High evidence and strong recommendation (IA)† |
|
|
Clinical practice guideline for physiotherapists |
Strong recommendation |
|
|
GOLD |
Evidence grade A‡ |
|
Dyspnea relief |
ACCP/AACVPR |
High evidence and strong recommendation (IA) |
|
|
Cochrane review |
Effect on the dyspnea domain of the CRQ§ was greater than the minimum clinically important difference |
|
|
GOLD |
Evidence grade A |
|
|
ACP systematic review, meta-analysis |
Average effect on the dyspnea domain of the CRQ was clinically significant |
|
Improved health-related quality of life |
ACCP/AACVPR |
High evidence and strong recommendation (IA) |
|
|
ACP clinical practice guideline, ACP systematic review |
PR programs improve health status |
|
|
GOLD |
Evidence grade A |
|
|
Clinical practice guideline for physiotherapists |
Strong recommendation |
|
|
Cochrane review |
Effect on all domains of the CRQ were greater than the minimum clinically important difference |
|
|
Meta-analysis |
Pooled difference in health status scores on the SGRQ was clinically significant* |
†Evidence comes from well-designed RCTs yielding consistent and directly applicable results: benefits clearly outweigh the risks and burdens; ‡GOLD RCTs: A = Rich body of data; B = Limited body of data; §For the CRQ health status questionnaire for COPD (with dyspnea, fatigue, emotion and mastery domains), an increase of 0.5 points per item or 10 points for total score is considered to be clinically significant; *for the SGRQ health status questionnaire, a 4-unit reduction (out of 100) is defined as a clinically noticeable improvement.
ACCP/AACVPR: American College of Chest Physicians/American Association of Cardiovascular and Pulmonary Rehabilitation; ACP: American College of Physicians; COPD: Chronic obstructive pulmonary disease; CRQ: Chronic Respiratory Questionnaire; GOLD: Global initiative for Obstructive Lung Disease;
PR: Pulmonary, rehabilitation; RCT: Randomized controlled trial; SGRQ: St George’s Respiratory
Questionnaire; IA: High evidence and strong recommendation.
A Comprehensive PR Program Incorporates the Following Components:
- Patient assessment and goal-setting
- Exercise and functional training
- Self-management (SM) education
- Nutritional intervention
- Psychosocial management
Effect of PR on Exercise Capacity, Symptoms and Health Status3
As per the current guidelines, COPD is classified into categories A, B, C and D, which takes into account the clinical assessment of symptoms and exacerbations, as well as lung function, which may be important indications for PR. A study was done to evaluate the effect of PR on exercise capacity, symptoms and health status in different COPD categories.
Results
One hundred sixty-seven subjects were included [COPD categories A (16%), B (12%), C (31%) and D (41%)].
Significant differences in most outcomes were found within each COPD category.
All COPD categories improved exercise capacity [6-minutes walking distance (MWD) and constant work rate]. Categories A and C had more distinct improvements in 6MWD compared to categories B and D. The proportion of subjects with a ≥ 35-m (minimum clinically important difference) increase in 6MWD was noted in 56.1%. Regarding 6MWD, values improved significantly in all COPD categories (Figure 2). There was a highly significant improvement in constant work rate (CWR) in all COPD categories (Figure 2).
In symptom control, as measured by Mahler’s index, it was found that COPD categories A and C improved significantly with the PR, but there was no significant change in the baseline and transitional dyspnea index in COPD categories B and D.
Global health status (St George Respiratory Questionnaire) improved significantly in all COPD categories.
Considering the intervention effect as the mean difference between post- and pre-PR outcome values, clinically and statistically significant effects were found for 6MWD (51.33 m), CWR (8.47 minute), dyspnea index (1.04) and St George Respiratory Questionnaire (–8.08), independent of COPD category, age, sex, body mass index and COPD-specific comorbidity test (COTE).
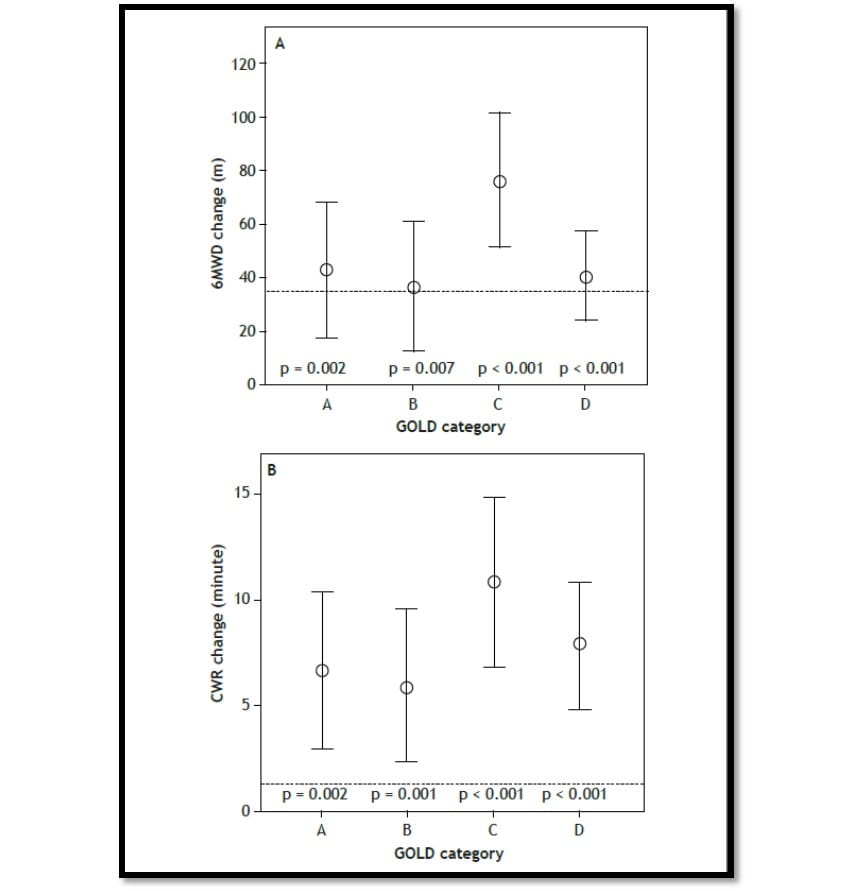
A: Change in 6-minute walking distance (6MWD); B: Change in constant work rate (CWR)
Conclusion
This study demonstrated that patients in all COPD categories may improve exercise capacity, symptoms and health status with PR programs and COPD categories alone may not be sufficient to discriminate which patients may benefit most from them.
Patient Assessment and Goal-setting4
Many health care professionals see their COPD patients every few months; but, patients have to deal with their disease on a regular basis. To improve outcomes in COPD patients, fostering a collaborative relationship between health care professionals,
COPD patients and their caregivers is required. Benefits in inpatient and outpatient setting may vary. Hence, proper arrangement and goal setting for the PR programs, must be done to achieve benefits as follows:
- In patients with chronic airway obstruction, improvements in exercise tolerance in inpatient PR programs gives similar results as outpatient PR programs but with a reduced cost in the inpatient setting.
- It becomes easier for the patients to talk to their healthcare providers when they keep a track of their symptoms, ultimately helping in the management of their condition.
- Talking to the family and health-care providers about trying to quit smoking can be beneficiary as family proves to be supportive, where the doctor will mention about the complications related to smoking and COPD.
- Discussing pulmonary rehab may help COPD patients learn how to breathe well and easily.
Evidence5
Defining minimal clinically important difference (MCID) of chronic obstructive pulmonary disease (COPD) health tools.
Introduction
Multiple tools are used in COPD to evaluate treatment effectiveness like Clinical COPD Questionnaire (CCQ), COPD Assessment Test (CAT) and St. George’s Respiratory Questionnaire (SGRQ). Hence, clinically relevant change as a consequence from questionnaires is of utmost importance. ‘The MCID defines to what extent change on a health status instrument is clinically relevant, which aids scientists and physicians in measuring therapy effects.’
Aim
A study first of its kind was conducted with a purpose to demonstrate the MCID of the CCQ, the CAT and the SGRQ in the same set of population undergoing PR using different approaches.
Methods
A total of 451 COPD patients (58 years, 65% male, 43 pack years, GOLD stage II/III/IV 50/39/11%) participated in a 3-week PR programme.
- Anchor-based approaches used to assess the MCID included:
- Patient-referencing
- Criterion-referencing
- Questionnaire referencing
- The distribution-based methods used to assess MCID included:
- Standard error of measurement (SEM)
- 1.96 SEM
- Half standard deviation (0.5 s.d.)
Results
- The MCID estimates obtained after
- Patient- and criterion-referencing were 0.56 and 0.62(CCQ); 3.12 and 2.96 (CAT); and 8.40 and 9.28 (SGRQ) (Table 2).
- Questionnaire-referencing were 0.28 – 0.61 (CCQ), 1.46 – 3.08 (CAT) and 6.86 – 9.47 (SGRQ)(Table 3).
- The SEM, 1.96 SEM and 0.5 s.d. were 0.29, 0.56 and 0.46 (CCQ); 3.28, 6.43 and 2.80 (CAT); 5.20, 10.19 and 6.06 (SGRQ).
- Pooled estimates revealed 0.52 (CCQ), 3.29 (CAT) and 7.91 (SGRQ) for improvement (Figure 3).
- The MCID score obtained was largely dependent on the type of method used and the score varied accordingly.
- For moderate to very severe COPD patients, the pooled results revealed clinically relevant improvements needing to exceed-
- 0.40 on the CCQ
- 3.00 on the CAT
- 7.00 on the SGRQ
|
Instrument |
No/hardly any improvement (GRC–1, 0 or +1) N = 98 |
Minimal improvement (GRC +2 or +3) N = 196 |
Moderate improvement (GRC +4 or +5) N = 123 |
Major improvement (GRC +6 or +7) N=25 |
|||||
|
|
∆a |
95% CIb |
∆a |
95% CIb |
∆a |
95% CIb |
∆a |
95% CIb |
|
|
COPD |
|||||||||
|
Symptoms |
-0.32 |
−0.54 to −0.10 |
−0.55 |
−0.70 to −0.40 |
−0.76 |
−0.96 to −0.56 |
−1.48 |
−1.97 to −0.99 |
|
|
Functional |
−0.27 |
−0.47 to −0.07 |
−0.55 |
−0.68 to −0.43 |
−0.78 |
−0.98 to −0.58 |
−0.97 |
−1.31 to −0.63 |
|
|
Mental |
−0.53 |
−0.84 to −0.22 |
−0.58 |
−0.78 to −0.38 |
−0.67 |
−0.94 to −0.39
|
−1.34 |
−1.84 to −0.84 |
|
|
Total |
−0.34 |
−0.52 to −0.15 |
−0.56 |
−0.68 to −0.44 |
−0.75 |
−0.92 to −0.58 |
−1.25 |
−1.54 to −0.96 |
|
|
CAT |
|||||||||
|
Total |
−2.05 |
−3.13 to −0.98 |
−3.12 |
−3.86 to −2.37 |
−3.67 |
−4.70 to −2.67 |
−6.44 |
−8.99 to −3.89 |
|
|
SGRQ |
|||||||||
|
Symptoms
|
−7.03 |
−10.86 to −3.19 |
−13.12
|
−16.05 to −10.19 |
−19.91 |
−23.92 to −15.90
|
−30.62 |
−38.40 to −22.84
|
|
|
Activities
|
−3.03 |
−5.28 to −0.78 |
−5.9
|
−7.88 to −4.08 |
−10.33 |
−12.78 to −7.87
|
−12.66
|
−18.69 to −6.62
|
|
|
Impact
|
−6.72 |
−9.57 to −3.86 |
−8.24
|
−10.14 to −6.33 |
−10.32
|
−12.77 to −7.87
|
−17.90
|
−23.64 to −12.16
|
|
|
Total |
−5.57 |
−7.79 to −3.35 |
−8.40 |
−10.07 to −6.73 |
−11.83 |
−14.00 to −9.66 |
−18.50 |
−22.81 to −14.18 |
|
COPD: Chronic Obstructive Pulmonary Disease; CAT: COPD assessment test; CCQ: Clinical COPD Questionnaire; CI: Confidence interval; GRC: Global rating of change; MCID: Minimal clinically important difference; SGRQ: St. George’s Respiratory Questionnaire; Δ: Change score.
aData were reported as mean change scores. Negative change represents improvement for all instruments. bPaired t-tests were applied to normally distributed variables and Wilcoxon signed-rank tests were used for not normally distributed data. Data were reported as 95% CI. All change scores were significant with p-value < 0.05.
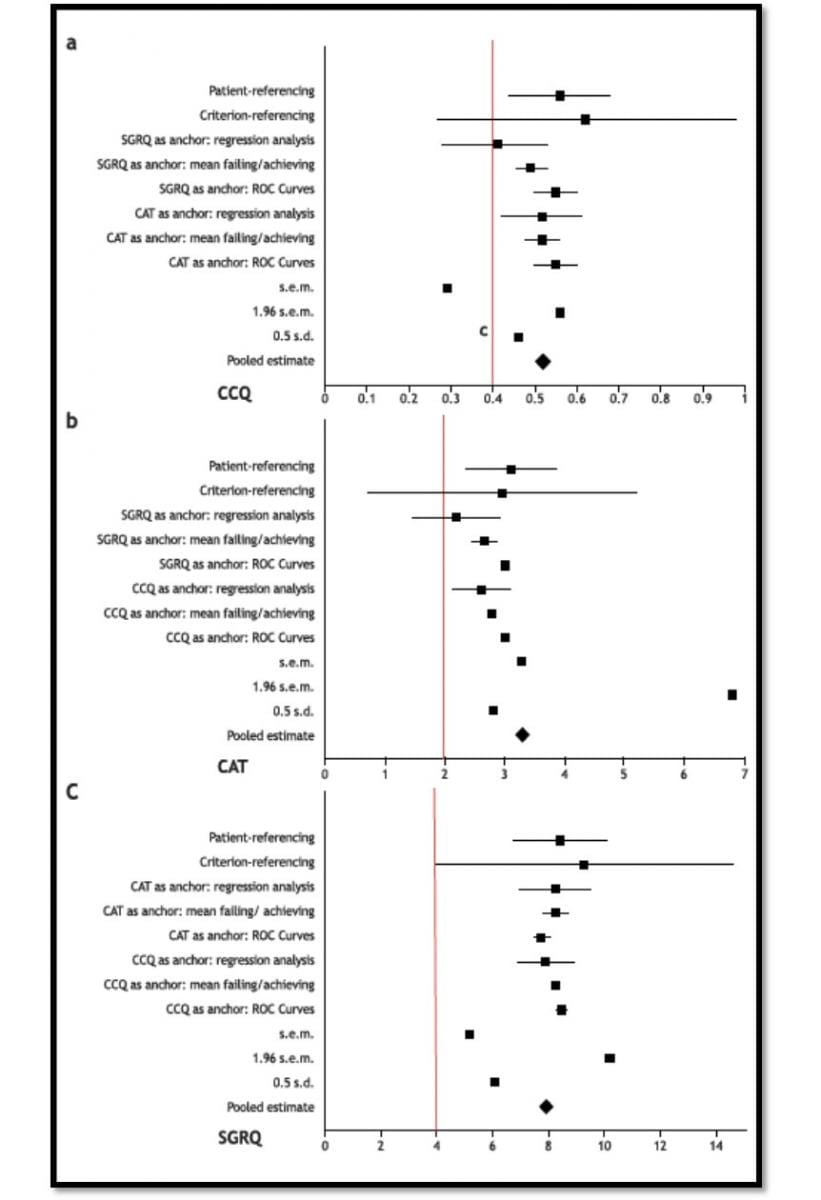
The horizontal plots represent the MCID estimates derived in this study, classified per method. Where appropriate the estimates include the 95% confidence interval. The red vertical line resembles the MCID estimate as obtained from the literature.
CCQ: Clinical COPD Questionnaire; CAT: COPD Assessment Test; SGRQ: St. George's Respiratory Questionnaire; MCID: Minimal clinically important difference; ROC: Receiver operating characteristics curves; SEM: Standard error of measurement; s.d.: Standard deviation.
|
|
Anchor CCQ = 0.40 |
Anchor CCQ = 0.50 |
Anchor CAT = 2 |
Anchor CAT = 3 |
Anchor SGRQ = 4 |
Anchor SGRQ = 7 |
|
Regression analysis |
||||||
|
CCQ |
— |
— |
0.48 (0.42–0.53) |
0.57 (0.53–0.61) |
0.34 (0.28–0.40) |
0.48 (0.44–0.53) |
|
CAT |
2.45 (2.14–2.77) |
2.81 (2.54–3.08) |
— |
— |
1.86 (1.46–2.27) |
2.61 (2.32–2.91) |
|
SGRQ |
7.51 (6.86–8.16) |
8.35 (7.79–8.90) |
7.73 (6.98–8.48) |
8.89 (8.31–9.47) |
— |
— |
|
Failing/achieving |
||||||
|
CCQ |
— |
— |
0.48 |
0.56 |
0.46 |
0.53 |
|
CAT |
2.74 |
2.82 |
— |
— |
2.45 |
2.86 |
|
SGRQ |
8.14 |
8.36 |
7.78 |
8.69 |
— |
— |
|
ROC curves |
||||||
|
CCQ |
— |
— |
0.50 AUC 0.767 Sens 0.701 Spec 0.706 |
0.60 AUC 0.771 Sens 0.716 Spec 0.710 |
0.50 AUC 0.796 Sens 0.750 Spec 0.714 |
0.60 AUC 0.802 Sens 0.763 Spec 0.730 |
|
CAT |
3.00 AUC 0.768 Sens 0.726 Spec 0.656 |
3.00 AUC 0.770 Sens 0.729 Spec 0.668 |
— |
— |
3.00 AUC 0.722 Sens 0.727 Spec 0.605 |
3.00 AUC 0.737 Sens 0.705 Spec 0.650 |
|
SGRQ |
8.30 AUC 0.817 Sens 0.777 Spec 0.703 |
8.63 AUC 0.816 Sens 0.787 Spec 0.702 |
7.50 AUC 0.719 Sens 0.659 Spec 0.656 |
8.00 AUC 0.745 Sens 0.673 Spec 0.681 |
— |
— |
Data are expressed as estimates (95% CI). N = 451.
AUC: Area under the curve; CAT: COPD Assessment Test; CCQ: Clinical COPD Questionnaire; COPD: Chronic obstructive pulmonary disease; ROC: Receiver operating characteristics curves; Sens: Sensitivity; Spec: Specificity; SGRQ: St. George’s Respiratory Questionnaire; 95% CI: 95% confidence interval.
Conclusion
The findings suggested that all improvements should be considered clinically relevant if they exceed 0.40 points on the CCQ, 3.00 points on the CAT and 7.00 points on the SGRQ in moderate to very severe COPD patients. These thresholds seem to be equivalent to MCID for domain scores on the SGRQ and CCQ.
Exercise and Functional Training6
Often, patients with COPD complain of exercise limitation. Clinicians can determine functional capacity using exercise testing, as it helps to provide a prognosis and to plan for therapeutic interventions.
- Lower extremity exercise training at a higher exercise intensity produces greater physiologic benefits than training at a lower intensity, in patients with COPD. Both low intensity and high-intensity exercise training produce clinical benefits for patients with COPD.
- Strength training is particularly beneficial in increasing the muscle strength and mass.
Evidence7
Respiratory muscle training with normocapnic hyperpnea (NH) improves ventilatory pattern and thoraco- abdominal coordination and reduces oxygen desaturation during endurance exercise testing in COPD patients.
Background
There is a limited availability of data about the effects of respiratory muscle training with NH in COPD.
Aim
A study was conducted to analyze the effects of NH on ventilatory pattern, exercise capacity and quality of life (QoL) in COPD patients.
Methods
- The study involved a total of 26 COPD patients (three females) between 49 to 82 years of age.
- The following tests were performed before and after NH-
- Spirometry
- Maximal inspiratory pressure (MIP)
- SGRQ
- 6-minute walk test (MWT)
- Symptom-limited endurance exercise test [endurance test to the limit of tolerance (tLim)] at 75% - 80% of peak work rate up to a Borg Score of 8 - 9/10
- To evaluate ventilatory pattern and thoracoabdominal coordination [phase angle (PhA)] during tLim, patients were provided with ambulatory inductive plethysmography.
- Subjects were trained at home for 4 weeks - 10 minutes, twice a day at 50% of maximal voluntary ventilation, after four supervised sessions.
- To maintain a Borg Score of 5 - 6/10, the workload was adjusted during the training session.
Results
- Out of 26, twenty subjects completed the study.
- After NH- (Figure 4)
- Maximal inspiratory pressure increased significantly (81.5 ± 31.6 vs. 91.8 ± 30.6 cm H2O, p < 0.01).
- Exercise endurance time (+150 seconds, p = 0.04) increased.
- 6-minute walk test (+30 meters, p = 0.03) increased.
- QoL (–8, p < 0.01) increased.
- During tLim, the ventilatory pattern changed significantly (lower ventilation, lower respiratory rate, higher tidal volume).
- Oxygen desaturation, PhA and dyspnea Borg Score were lower for the same work intensity [p < 0.01, p = 0.02 and p < 0.01, respectively; one-way analysis of variance (ANOVA)](Figure 5).
- The improvement in tidal volume and oxygen saturation after NH were significantly related (R2 = 0.65, p < 0.01).
Conclusion
Based on the findings, it was brought to understanding that NHimproves inspiratory muscle performance, exercise capacity and QoL. New findings were encountered in terms of significant change in ventilatory pattern, which improves oxygen saturation and an improvement in thoracoabdominal coordination (lower PhA). The above two findings have an important role to play in the explanation of reduced dyspnea during the endurance test. All the above factors account for an improved exercise capacity after NH training.
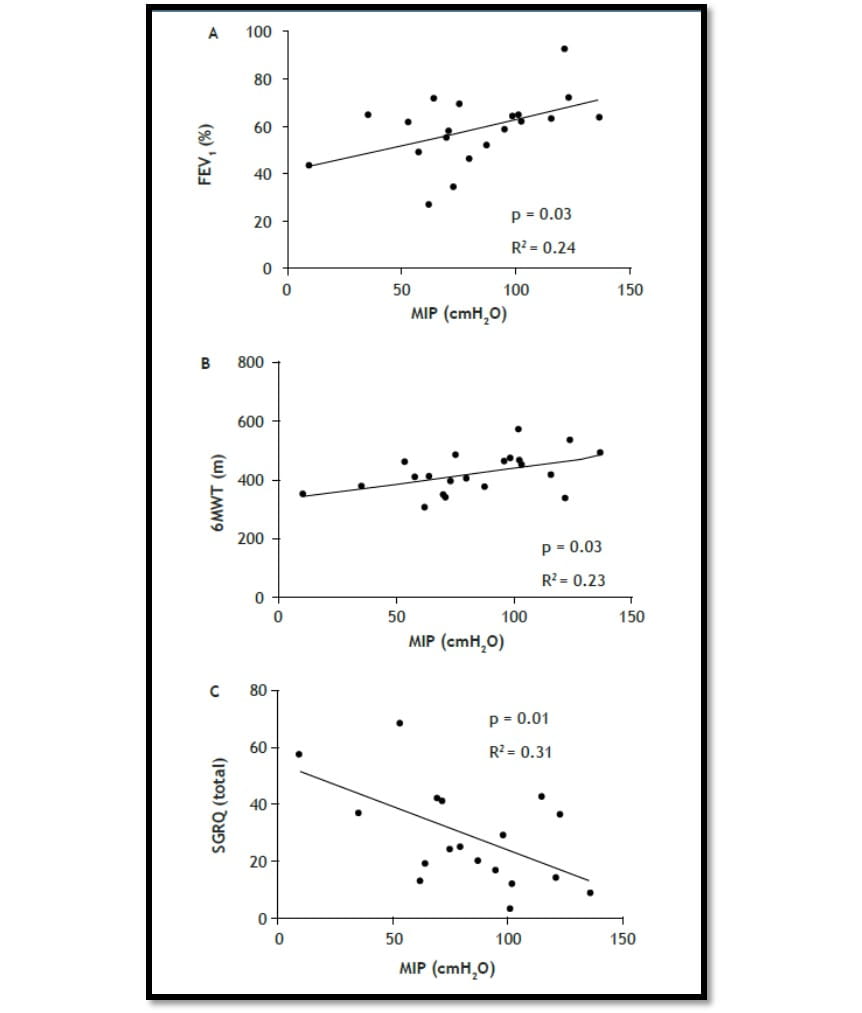
FEV1: Forced expiratory volume 1; 6MWT: 6-minute walk test; SGRQ: St. George Respiratory Questionnaire; MIP: Maximal inspiratory pressure.
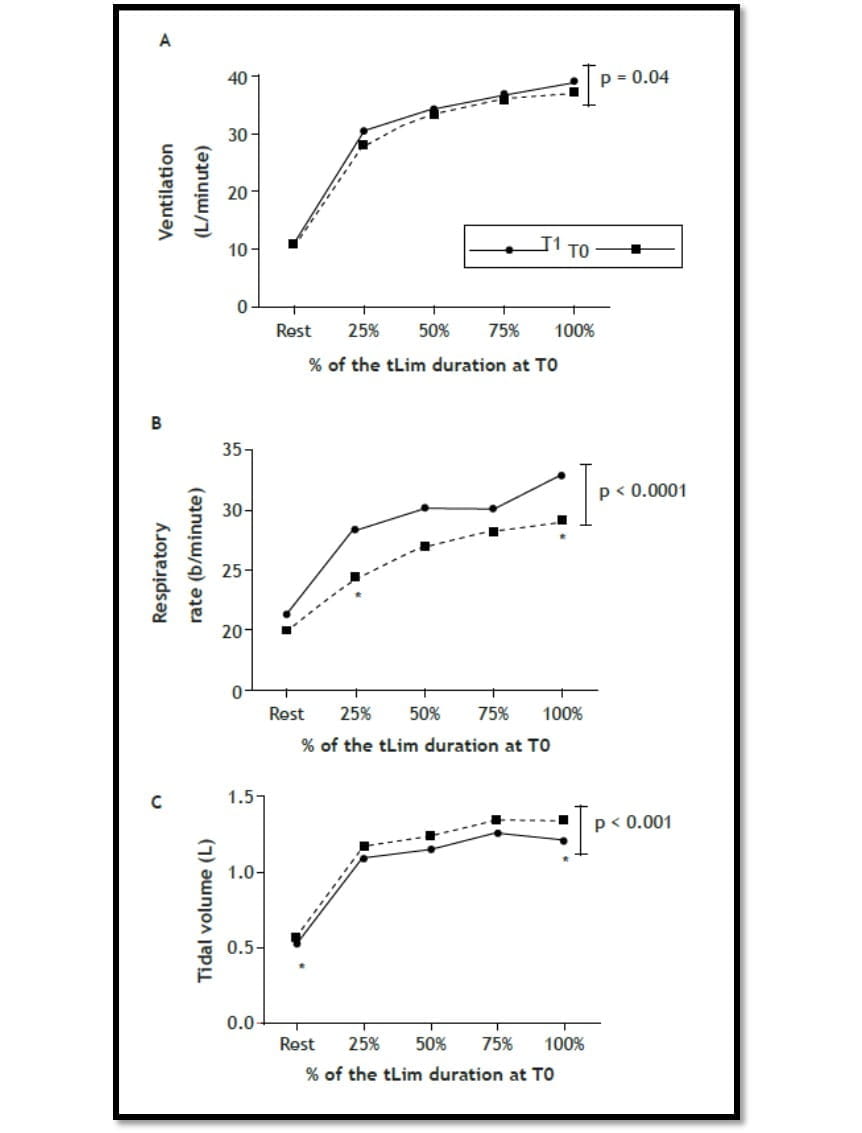
tLim: Endurance test to the limit of tolerance; T0: Baseline; T1: After 4 weeks of respiratory muscle training.
Self-Management Education8
There are many factors that may affect a patient’s ability to self-manage (e.g. severity, presence of comorbidities, depression, education, psychological factors and ethnicity). One behavioural model that describes self-management (SM) is patient activation, which emphasises that patients should have the knowledge, skills and confidence to manage their own health and healthcare. Interventions to promote SM should aim to address each of these components.
Benefits of SM support
Self-management support helps patients gain the required knowledge and skills for:
- Managing the medical regimens
- Changing the health behaviour
- Controlling and improving the disease state and hence enhancing the well-being
Patient education alone is not sufficient; monitoring and assessment of progress is also essential. SM interventions should teach skills that promote health behaviour modification with the aim of increasing self-efficacy (the belief that one can successfully execute particular behaviours), thus improving clinical outcomes, including adherence. Strategies to promote self-efficacy include personal experience and practice, feedback and reinforcement, analysis of causes of failure and shared experience with successful peers.
SM programmes can be delivered in a number of ways (e.g. series of workshops, written material, by telephone, internet or a combination) by various professionals or lay personnel and can have a range of components.
Evidence9
Factors influencing patient participation in COPD programmes.
Introduction
The COPD support programmes consisting of studies of SM and PR programmes often encounter with the problem of poor patient participation. It is very important to understand this problem beyond the previously reported socio-demographics and clinical factors.
Aim
This study was conducted with an aim to analyse various factors that describe patient participation in studies of COPD support programmes.
Methods
- Literature published from 1984 to 1st February 2015 was collected and thematic framework synthesis was conducted on it.
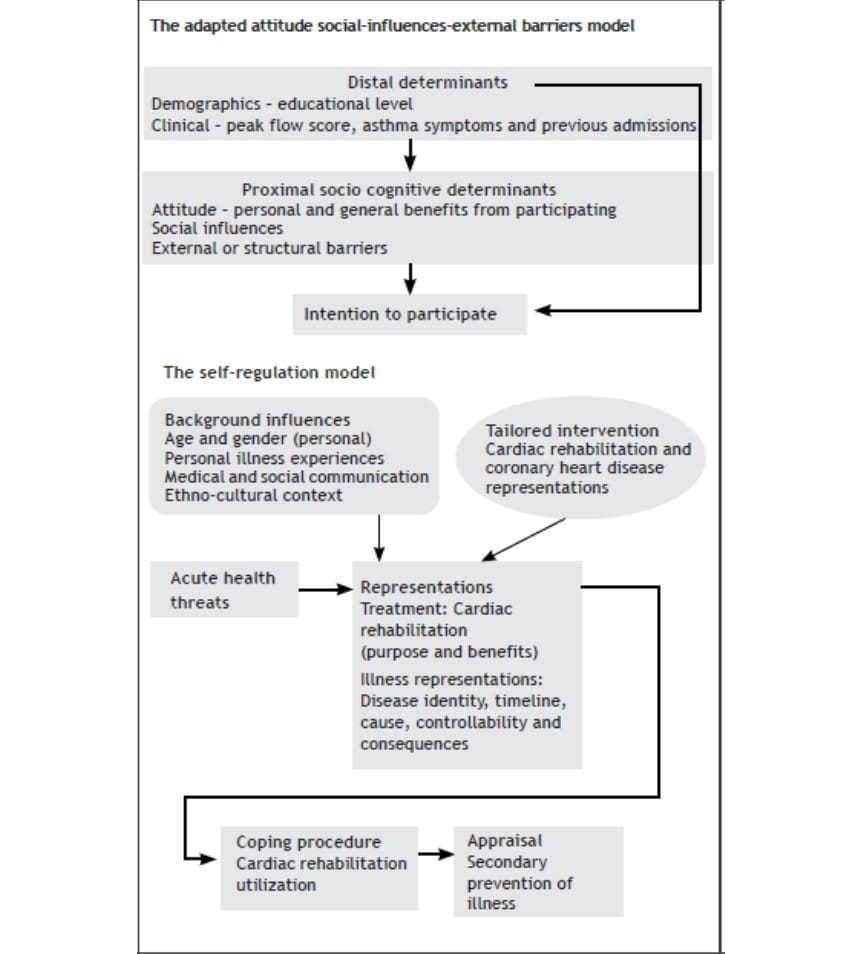
- Adapted ‘attitude-social influence-external barriers’ and the ‘self-regulation’ models were created and emergent themes and sub themes were recorded in detail onto them to produce analytical themes.
Results
- A total of 10 studies out of 12 were included in PR (n = 9) and SM (n = 1).
- Three descriptive themes and 38 sub-themes were recorded onto models, leading to the production of four analytical themes (Figure 6):
- Attitude
- Social influences
- Illness
- Intervention representations
The influencing factors are shown in the table below:
|
Factor number |
Factor |
|
1. |
Attendance-helping oneself through health improvements, perceived control of worsening condition, perceived benefits and positive past experience of the programme, as well as perceived positive influence of professionals. |
|
2. |
Non-attendance-perceived negative effects and negative past experience of the programme, perceived physical/ practical concerns related to attendance, perceived severity of condition/symptoms and perceived negative influence of professionals/friends. |
|
3. |
Dropout-no health improvements perceived after attending a few sessions of the programme, perceived severity of the condition and perceived physical/practical concerns related to attendance. |
COPD: Chronic obstructive pulmonary disease.
Conclusion
Patient’s participation in COPD support programmes was influenced by psychosocial factors including perceived practical/ physical concerns related to attendance, sometimes driven by beliefs. Behaviour change interventions targetting negative beliefs/perceptions may be useful to improve participation in COPD support programmes and patient outcome in the long run.
Nutritional Intervention10
Being underweight has been found to be a poor prognostic sign in COPD. It is also clear that undernutrition is at least in part associated with the severity of airflow obstruction.
- Nutritional support leads to improved exercise performance and enhancement of exercise rehabilitation programmes.
- Nutritional support in COPD results in significant improvements in a number of clinically relevant functional outcomes like nutritional intake and weight.
- A carefully planned nutrition program can reverse undernutrition in patients with COPD, at least over the short term.
- Successful nutritional repletion can lead to improvement in exercise performance and respiratory muscle function.
Evidence11
Effect of nutritional supplement along with PR in COPD management.
Aim
The aim of this study was to analyze the effects of nutritional supplementation along with PR on factors like HRQoL, anxiety and depression, mid thigh cross-sectional area (CSA), dyspnea, body composition and the exercise capacity in patients with advanced COPD.
Results
- Patients showed an improvement in the HRQoL, dyspnea, anxiety and the exercise capacity in the PRNS group.
- There were significant improvements in the mid-thigh CSA and lean body mass in the PRNS group only (Figure 7 see page 25).
Conclusion
Combining PR with nutritional supplementation leads to significant improvements in the mid-thigh CSA and lean body mass. Hence, with this evidence, the study suggests that nutritional supplementation along with PR programs can help alleviate weight loss and muscle wasting in the COPD patients.
Psychosocial Management2
Anxiety and depression are important comorbidities of COPD and a significant proportion of COPD patients referred to PR centers, suffer from these psychiatric disorders.
- Psychological support can help patients to reduce their negative emotions, which in turn, may improve compliance with PR.
- Psychological support helps in overcoming addictions, especially tobacco smoking and, along with medical treatment for smoking cessation, is an important intervention in PR programs.
- PR has certainly been demonstrated to provide beneficial effects on dyspnea, improvement in muscle strength and endurance, improvement of psychological status, reduction of hospital admissions and improvement of HRQoL in COPD patients, with a gradual increase in daily physical activity and autonomy.
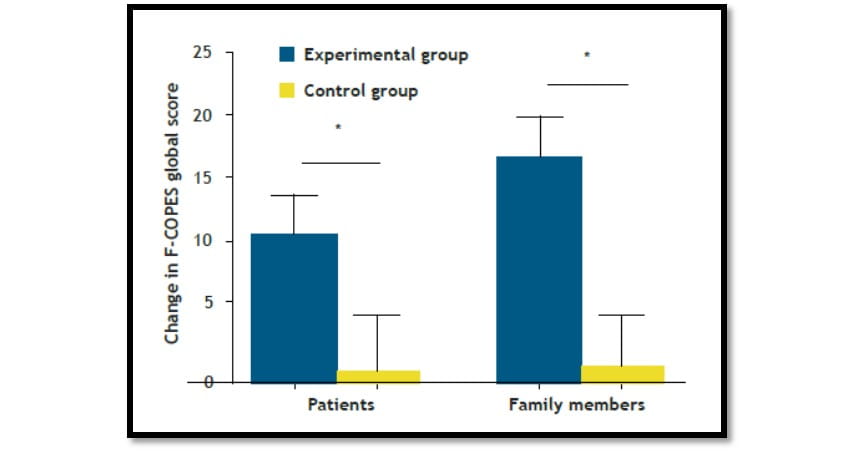
Data are presented as mean ± SE. Significant differences are identified with* (p < 0.05). F-COPES: Family Crisis Oriented Personal Scales.
Evidence12
Family-based PR programme and its psychosocial impact on patients and family members in COPD management.
Introduction
Psychosocial intervention has been suggested as a potentially effective supplement to medical treatment in COPD. Moreover, involving family as a part of this management plan is thought to further improve the quality of COPD management.Aim
The aim of this study was to understand that while managing COPD, how family intervention during PR programs affects the patients as well as the coping strategies of the family members.
Results
The outcomes of the randomized controlled trial showed significant improvements in the experimental (family-based) group.
- Patients (p = 0.048) and family members (p = 0.004) in this group had improved family coping as compared to the control (Figure 8).
- Family members of this group also showed significant improvements in the psychological distress (p = 0.033) as well as their sexual relationships (p = 0.026).
- Patients in this group also showed marked improvements in their functional balance, knee extensors strength and exercise tolerance.
- Patients also demonstrated an enhanced HRQoL after the intervention.
Conclusion
The current study provided evidence and supported the benefits of family-based programs to manage COPD in patients. The study also demonstrated that the intervention of family in such PR programs will only enhance the coping strategies of the family members and the patients. Further, the patients will also benefit by having an improved HRQoL.
Summary
Key Points
- Globally by 2030, COPD is projected to become the third leading cause of death.
- PR is recommended for all symptomatic COPD patients, regardless of severity and involves exercise training, patient education, nutritional advice and psychosocial support.
- To improve outcomes in COPD patients, fostering a collaborative relationship between health care professionals, COPD patients and their caregivers is required.
- This three-point triangular relationship requires mutual feedback and positive reinforcement in a non-judgemental environment.
- Clinicians can determine functional capacity using exercise testing, as it helps provide a prognosis and to plan for therapeutic interventions.
- Several modalities of exercise tests for patients with COPD include the 6MWT, stair-climbing test, shuttle test (incremental and endurance), cardiopulmonary exercise test (CPET) and cardiac stress test.
- Exercise training, the cornerstone of PR, has been shown to improve dyspnea and HRQoL and decrease healthcare use.
- Past ten years of research has clearly documented in COPD patients, dyspnea, exercise tolerance and QoL can be improved considerably with appropriate therapeutic interventions.
- SM programmes can be delivered in a number of ways (e.g. series of workshops, written material, by telephone, internet or a combination) by various professionals or lay personnel and can lead to significant improvement in thelife of a COPD patient.
- Successful nutritional repletion have been shown clinically in these patients to improve exercise performance and respiratory muscle function.
- Psychosocial treatments as supplements to standard medical treatment may potentially benefit the large group of patients with COPD who struggle with massive problems which so far unfortunately have been neglected.
- The rationale of combining pharmacological and nonpharmacological therapies is strong and multiple levels of synergistic interactions between these two approaches have been reported.
References
1. Garvey C. Recent updates in chronic obstructive pulmonary disease. Postgrad Med.
2016;128(2):231-8.
2. Corhay JL, Dang DN, et al. Pulmonary rehabilitation and COPD: providing patients a good environment for optimizing therapy. Int J Chron Obstruct Pulmon Dis. 2014;9:27-39.
3. Alfarroba S, Rodrigues F, et al. Pulmonary Rehabilitation in COPD According to Global Initiative for Chronic Obstructive Lung Disease Categories. Respir Care. 2016 Oct;61(10):1331-40.
4. Clini E, Foglio K, et al. In-hospital short-term training program for patients with chronic airway obstruction. Chest. 2001 Nov;120(5):1500-5.
5. Alma H, de Jong C, et al. Health status instruments for patients with COPD in pulmonary rehabilitation: defining a minimal clinically important difference. NPJ Prim Care Respir Med. 2016 Sep 1;26:16041.
6. Ries AL, Bauldoff GS, et al. Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based
Clinical Practice Guidelines. Chest. 2007 May;131(5 Suppl):4S-42S.
7. Bernardi E, Pomidori L, et al. Respiratory muscle training with normocapnic hyperpnea improves ventilatory pattern and thoracoabdominal coordination, and reduces oxygen desaturation during endurance exercise testing in COPD patients. Int J Chron Obstruct Pulmon Dis. 2015 Sep 10;10:1899-906.
8. Jordan RE, Majothi S, et al. Supported self-management for patients with moderate to severe chronic obstructive pulmonary disease (COPD): an evidence synthesis and economic analysis. Health Technol Assess. 2015 May;19(36):1-516.
9. Sohanpal R, Steed L, et al. Understanding patient participation behaviour in studies of COPD support programmes such as pulmonary rehabilitation and self-management: A qualitative synthesis with application of theory. NPJ Prim Care Respir Med. 2015 Sep 17;25:15054.
10. King DA, Cordova F, et al. Nutritional aspects of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008 May 1;5(4):519-23.
11. Gurgun A, Deniz S, et al. Effects of nutritional supplementation combined with conventional pulmonary rehabilitation in muscle-wasted chronic obstructive pulmonary disease: a prospective, randomized and controlled study. Respirology. 2013 Apr;18(3):495-500.
12. Marques A, Jacome C, et al. Family-based psychosocial support and education as part of pulmonary rehabilitation in COPD: a randomized controlled trial. Chest. 2015 Mar;147(3):662-672.