

Allergic Rhinitis and Rhinosinusitis: The Link



Allergic Rhinitis: Not Just a Runny Nose!
According to the Allergic Rhinitis and its Impact on Asthma (ARIA 2008) document, allergic rhinitis is defined as an inflammation of the lining of the nose and is characterized by nasal symptoms including rhinorrhoea, sneezing, nasal blockage and/or itching of the nose.1
Allergic rhinitis (AR) is a major chronic respiratory disease, affecting 18% to 40% of adults worldwide, diagnosed by history, physical examination and objective testing.2 According to ARIA, AR affects 500 million people worldwide and over 100 million in India, Pakistan and surrounding countries.1 AR develops before the age of 20 years in 80% of cases, peaking in adolescence.3
To add to this huge burden of AR, evidences suggest that the prevalence is further increasing.4 Apart from the classical symptoms of sneezing, rhinorrhoea and nasal congestion, severe AR has been associated with significant impairments in how patients function in day-to-day life, affecting their quality of life (QOL), sleep and work performance.1
A noteworthy feature of this disease is that, AR is rarely found in isolation and should be considered in the context of systemic allergic diseases. The presence of AR is associated with numerous comorbid disorders such as asthma, otitis media with effusion, rhinosinusitis and sleep disturbances.5
Poorly controlled AR can develop or trigger exacerbations of these comorbidities because they often share pathophysiologic pathways in common with AR.6
When AR involves the sinuses, it is referred to as rhinosinusitis.7 The term ‘rhinosinusitis’ rather than ‘sinusitis’ reflects more accurately the close anatomical and pathophysiological relationship between AR and chronic sinusitis, which are commonly comorbid.8 Infectious AR is also known as rhinosinusitis.1 Thus, rhinosinusitis is defined as inflammation of the nose and paranasal sinuses. Acute rhinosinusitis is usually infectious, whereas chronic rhinosinusitis is less clearly infectious and often more inflammatory.9 AR and rhinosinusitis usually coexist and are concurrent in most individuals.
In a study conducted in Indian population, incidence of sinusitis was as high as 22.8% in patients with AR.10 Both AR and rhinosinusitis can significantly decrease a patient’s QOL, aggravate comorbid conditions and require significant direct medical expenditures.11
Allergic Rhinitis and Chronic Rhinosinusitis: Prevalence and Clinical Impact
Chronic rhinosinusitis (CRS) constitutes one of the commonest conditions encountered in clinical practice and may present to a wide range of clinicians from primary care to pulmonologists, allergists, otorhinolaryngologists and even intensivists when severe complications occur.12
Patients who are afflicted with allergies have a predisposition for developing sinusitis. It has been demonstrated that both disorders exist in the same patient 25% to 70% of the time.13
A study conducted in 2012 found that 72 out of 121 patients with chronic nasal symptoms and positive skin tests for allergies had positive sinus computed tomography scans showing the presence of sinusitis.13
AR may be a contributing factor in 25% to 30% of patients with an acute maxillary sinusitis and in as many as 60% to 80% of patients with CRS. In a recent analysis of medical claims data, 26% of patients with sinusitis had concomitant AR.
Also, AR was majorly found to be a contributing factor in as many as 60% to 80% of patients with chronic sinusitis.14
The burden of both these diseases, i.e., AR and CRS in terms of direct costs to the healthcare system is tremendous. Reflective of their associated healthcare disease burdens, both CRS and AR impart a substantial burden on individual QOL on affected subjects. A study conducted at the division of otolaryngology at Massachusetts sought to examine the QOL burdens of AR and CRS in terms of functional limitations and the number of work day’s lost.15 According to this study; aggregate workdays missed in the United States were estimated as 11.5 million and 10.7 million for CRS and AR, respectively. These figures further emphasize on the substantial societal burden of these upper respiratory diseases. CRS is associated with more workdays lost than AR. Thus, both CRS and AR impart significantly increased odds ratios for activity, work and social limitations.15
The Link between Allergic Rhinitis and Rhinosinusitis
The symptoms of AR and rhinosinusitis overlap and rhinosinusitis rarely occurs in the absence of AR.16 AR and rhinosinusitis may have a common underlying pathology.14
The following pointers will help define the association between AR and rhinosinusitis.
- Sinusitis often precedes by AR and rarely occurs without concurrent AR.17
- The symptoms, nasal obstruction/discharge and loss of smell occur in both disorders.17
- Patients afflicted with allergies have a predisposition for developing sinusitis.13
- The aggregation of research suggests that AR and rhinosinusitis are linked by the united allergic airway, a notion that encompasses commonalities in pathophysiology, epidemiology and treatment.13
- The etiology of the link between AR and rhinosinusitis is multifactorial.13
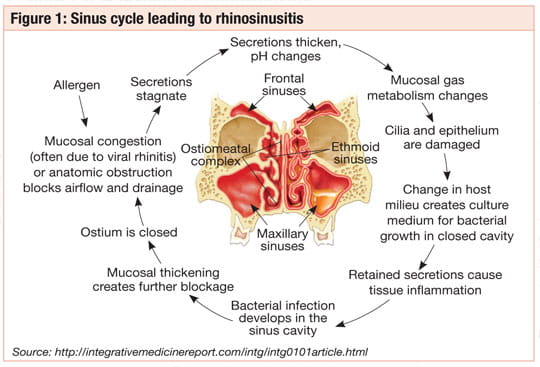
- Firstly, anatomically, patients with AR have edematous nasal mucosa, damaged nasal cilia and overproduction of secretions, which could lead to a blockage of ostial drainage of the sinuses. This blockage results in stagnant debris and secretions.13
- Likewise, chronic inflammation due to allergies can lead to obstruction and subsequent sinusitis.17
- The catalyst relating the two disorders is thought to involve nasal sinus overflow obstruction, followed by bacterial colonization and infection leading to acute, recurrent or chronic rhinosinusitis17 (Figure 1).
- Secondly, there is an important interrelationship between the middle turbinate and the ethmoid sinus such that cyclic variations in nasal turbinate swelling occurring during the normal nasal cycle can cause mucosal thickening. This thickening might be interpreted as ethmoid sinusitis. The ethmoid infundibulum and the nose represent contiguous structures sharing vascular, neuronal and interconnecting anatomic pathways.16
- Various medical researchers have supported the close relationship between AR and sinusitis. A review of patients (4 to 83 years of age) who had surgery to treat their chronic sinus conditions revealed that those with seasonal allergy are more likely to experience a recurrence of their sinusitis.17
The evidences of a common pathophysiological mechanism between AR and CRS are convincing. Although, a clear causal mechanism leading from AR to development of CRS remains to be elucidated, an increasing number of studies have shown the possibility and evidence of this link.
Factors Causing Chronic Rhinosinusitis
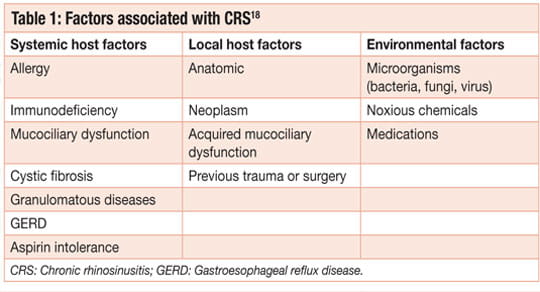
Regarding the etiology of CRS, numerous hypotheses have been proposed with a great deal of overlap, supporting a multifactorial basis. Currently, rhinosinusitis is believed to arise primarily from persistent inflammation of the mucosa and perhaps the underlying bone.
Possibly, the most appropriate broad classification of predisposing factors for CRS is into host and environmental factors (Table 1).18
Diagnosis of Chronic Rhinosinusitis
The diagnosis of CRS is broadly based on clinical symptoms and objective evaluation. Symptoms must be present for at least 12 consecutive weeks. Nasal obstruction, facial pressure/congestion/fullness, discolored nasal discharge and hyposmia are the signs and symptoms used to diagnose CRS (Table 2).18
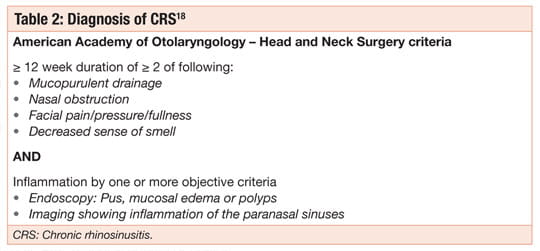
Several studies have shown using symptoms alone to diagnose CRS can be nonspecific. Therefore, nasal endoscopy or imaging must also be used to confirm the presence of sinonasal disease. Endoscopic findings suggestive of CRS include mucopurulent discharge, nasal polyps or polypoid change and/or mucosal edema obstructing the middle meatus. A recent study found the addition of endoscopic findings to symptom-based criteria significantly improved diagnostic accuracy of CRS.18
Computed tomography (CT) is considered the gold standard for imaging in CRS. Findings consistent with CRS include isolated or diffuse mucosal thickening, bone changes or air-fluid levels.18
Patients with CRS may frequently present with associated diagnoses of asthma, allergy, dental disease, nasal polyposis, ciliary dyskinesia, cystic fibrosis and immunodeficiency syndromes. Thus, CRS represents a spectrum of diseases with a range of appropriate treatments. Once the diagnosis of CRS has been established, workup and treatment of patients must be individualized.18
Chronic Rhinosinusitis: Clinical Management Strategies
Although the American Academy of Otolaryngology – Head and Neck Surgery guidelines state CRS should be treated with “maximal medical therapy,” there is no such standardized therapy for CRS. This is in part due to the heterogeneity of the disease, which includes CRS with nasal polyps (CRSwNP), CRS without nasal polyps (CRSsNP), allergic fungal rhinosinusitis (AFS) and CRS associated with other systemic diseases such as atopy, asthma, cystic fibrosis and aspirin-exacerbated respiratory disease (AERD).
Symptoms may be mild with little effect on QOL or may result in significant health problems and loss of productivity. As such, maximal medical therapy is best considered as a philosophical approach, in which CRS in a given individual is treated with a combination of medical strategies best suited for that patient.18
Current treatment strategies aim to reduce inflammation with the goal of restoring normal sinus physiology.
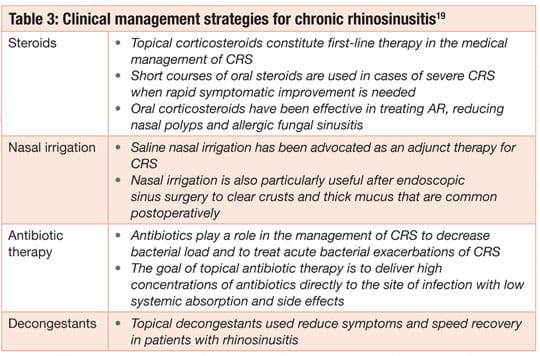
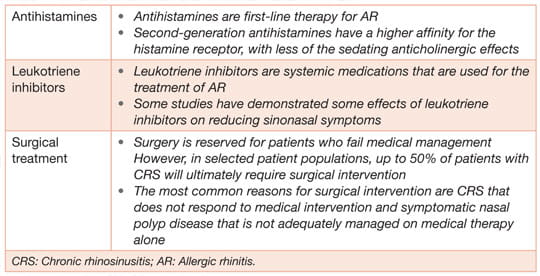
As described in Table 3, these treatment strategies include topical and systemic medications. Surgery is performed for recalcitrant disease refractory to medical therapy.19
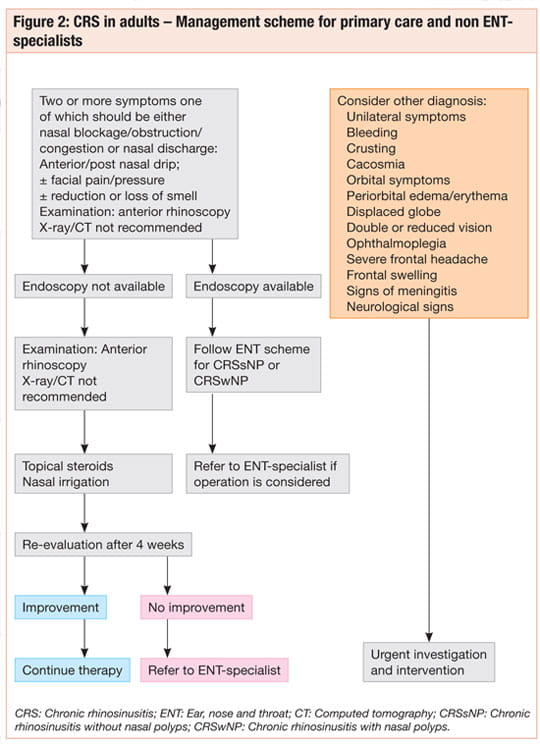
Management Scheme for Adults with Chronic Rhinosisnusitis for Primary Care and Non-ENT Specialists 20
As per Figure 2, CRS usually includes the presence of 2 or more signs or symptoms lasting more than 12 weeks, with or without acute exacerbations, one of which should be either nasal blockage/obstruction/congestion or nasal discharge (anterior/posterior nasal drip):
- ± Facial pain/pressure
- ± Reduction or loss of smell
Initial treatment for these patients will be depending on the severity of disease. Acute exacerbations of CRS should be treated like acute rhinosinusitis. Generally, these patients should be treated with nasal irrigation and topical steroids, if symptoms improve therapy should be continued otherwise patients should be referred an ENT specialist.
Conclusion
AR is a highly prevalent atopic disorder and it often coexists with rhinosinusitis. The aggregation of research suggests that AR and rhinosinusitis are linked by the united allergic airway. The etiology of the link between AR and sinusitis is likely multifactorial. Further, AR as well as CRS have a significant impact on patients’ QOL and associated with illness-related productivity loss in the workplace. Patients who have AR and sinusitis face significant morbidity as well as higher medical costs.
Thus, suggested approach would be to evaluate the underlying allergies in a patient with CRS. However, significant advances in medical and surgical therapy have not only reduced morbidity and improved the overall results of intervention but also provided long-term benefit when effectively combined. Current treatments aim to reduce inflammation with the goal of restoring normal sinus physiology.
Key Points
- The symptoms of allergic rhinitis and sinusitis overlap and sinusitis rarely occurs in the absence of allergic rhinitis.
- AR as well as CRS have a significant impact on patients’ QOL and associated with illness-related productivity loss in the workplace.
- Maximal medical therapy is best considered as a philosophical approach, in which CRS in a given individual is treated with a combination of medical strategies best suited for that patient.
- Current treatment strategies aim to reduce inflammation with the goal of restoring normal sinus physiology.
References
- Allergy. 2008; 63 Suppl 86:8-160.
- J Aller Ther. 1:103. doi:10.4172/2155-6121.1000103.
- J Allergy Clin Immunol. 2008; 122:S1-84.
- Allergy Asthma Clin Immunol. 2011, 7(Suppl 1):S3.
- J Allergy Clin Immunol. 2001; 108(1 Suppl):S9-15.
- Korean J Med. 2013; 85(5):457-462.
- PCRJ editorial. 2011; 20(1): 11-12.
- Comorbidities of Allergic Rhinitis, Allergic Diseases - Highlights in the Clinic, Mechanisms and Treatment, Prof. Celso Pereira (Ed.), ISBN: 978-953-51-0227-4, InTech.
- J Allergy Clin Immunol. 2004; 114: 115-212.
- Indian J Otolaryngol Head Neck Surg. 2009; 61:5–8.
- J Allergy Clin Immunol. 2010 Feb; 125(Suppl 2):S103-15.
- Ann Afr Med. 2010; 9:20-26.
- Am J Rhinol Allergy. 2012; 26(3):187–90.
- J Manag Care Pharm. 2004; 10(4):310-17.
- Am J Rhinol Allergy. 2012; 26(2):120–2.
- http://allergycliniconline.com/2012/04/05/differential-considerations-for-rhinitis-and-rihonosinusitis/
- http://entcenterutah.com/fact-sheet-allergic-rhinitis-sinusitis-and-rhinosinusitis/
- Infect Drug Resist. 2013; 6:1-14.
- Proc Am Thorac Soc. 2011; 8:132–40.
- Rhinology. 2012; 50(Suppl 23):1-298.












