

Treating Benzodiazepine Refractory Convulsive Status Epilepticus in Children: Levetiracetam vs. Fosphenytoin

19 Mar, 21


Introduction
The incidence of status epilepticus (SE) in pediatric patients, particularly in children aged less than 5 years is high in developing countries. Benzodiazepine resistance is common in SE patients, and phenytoin is conventionally used as the first-line therapy in children in such cases. With a better safety profile, levetiracetam scores over fosphenytoin as a second-line agent. Very few studies have compared the efficacy and safety of levetiracetam and fosphenytoin in pediatric patients with SE.
Aim
- To compare the clinical effectiveness of levetiracetam with fosphenytoin to control Benzodiazepine Refractory Status Epilepticus (BRSE) in children
- To compare the acute drug related side-effects and ventilation requirement associated with both the anti-epileptic drugs
Patient Profile
- Children hospitalized for BRSE in tertiary care centre in southern India (age; 2 months-18 years; n=61)
Methods
Study Design
- Open-label, randomized, comparative trial
Treatment Strategy
- Patients were randomized as follows:
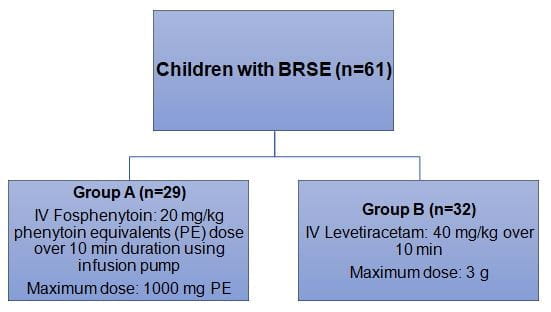
- Patients were observed for next 20 min for clinical termination of seizure activity and response latency
- Compliance medication after discharge was as follows:
- Group A: Oral phenytoin; 5-10 mg/kg/day in two divided doses
- Group B: Oral levetiracetam; 30 mg/kg/day in two divided doses
Outcomes
- Time to terminate seizure (response latency)
Results
- Median age of the study population was 17 months. The baseline demographics were comparable in both the study groups.
- Nearly 81.9% patients (n=50) had seizure control with either levetiracetam or fosphenytoin, 11 children required additional AEDs to control seizure. The number of additional antiepileptic drugs (AEDs) required for seizure termination was significantly higher in group A vs. group B (31% vs. 7%; p=0.0001)
- Time to secure IV line was faster in levetiracetam group vs. fosphenytoin group (2.5 min vs. 3.1 min)
- Time to seizure termination (response latency) was lower in group B vs. group A (13.3 min vs. 16.2 min; p=0.07). The seizure recurrence at 6 h and 24 h did not differ significantly in both the study groups
- Fifty-eight patients (98%) required Pediatric Intensive Care Unit (PICU) admission and among those 5 (8.2%) children required mechanical ventilation. Duration of PICU stay and hospital stay did not differ significantly in both the study groups.
- There were no reports of adverse events such as hypotension and arrhythmia in either of the study groups.
Conclusions
- Levetiracetam appeared to be an effective alternative to fosphenytoin for managing BRSE in children
- Large-scale, multicentric trials are warranted to verify these findings.
Indian J Pediatr. 2020;87(7):512–19.

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
21 May, 26

21 May, 26
Journal Scans
18 May, 26

18 May, 26
Journal Scans
15 May, 26
15 May, 26


