

STEPP-AMI Two-Year Follow-up: Pharmacoinvasive Strategy vs. Primary PCI in Indian STEMI Patients

26 Sep, 16


Introduction
Implementing a pharmacoinvasive strategy (initial bolus lysis followed by appropriate percutaneous coronary intervention [PCI]) might alleviate various barriers that delay the reperfusion of ST-segment elevation myocardial infarction (STEMI), particularly in a developing country like India.
Aim
To determine the safety, efficacy and feasibility of pharmacoinvasive strategy vs. primary PCI (PPCI) in STEMI patients at 2 years
Patient Profile
- Patients with STEMI presenting within 12 h of onset of symptoms and requiring a reperfusion strategy (n=200; age, 18-75 years)
Method
Study Design
- Prospective, observational, multicenter pilot study
Treatment Strategy
Primary Endpoint
- A composite of death, cardiogenic shock, reinfarction, repeat revascularization, and congestive heart failure at 30 days and followed up till 2 years
Safety endpoints
- Bleeding endpoints assessed using the TIMI classification at 30 days and till 2 years
Results
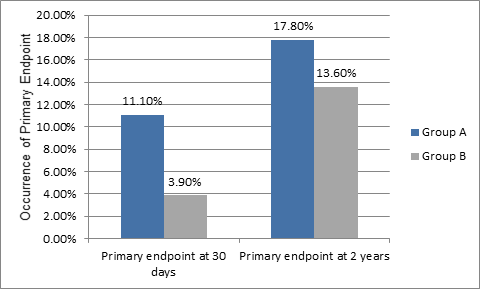
- Incidence of primary endpoint was similar in pharmacoinvasive and primary PCI groups at 2 years (17.8% vs. 13.6%, relative risk (RR)=1.31; p=0.47) (Figure 1)
- Primary endpoint remained similar in both the groups even after adjustment for age, sex & Killip's class (at end of 2 years: 17.8% vs. 13.6%, RR=1.15; p=0.69
- Bleeding risk did not differ significantly in the study groups (2.2% vs. 0.6%; p=0.4)
Figure 1: Occurrence of primary endpoint in the study groups
Conclusion
- Prompt pharmacoinvasive strategy is similar to PPCI in terms of efficacy and safety even at the end of 2 years
- The findings support the approach of adopting a pharmacoinvasive strategy in the settings where patient and system-related delays are inherent
Indian Heart J 2016; 168: 169-73

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


