

Significance of Secondary Resection and Efficacy of BCG Strains in Intermediate/High-Risk Non-Muscle-Invasive Bladder Cancer

1 Oct, 21


Introduction
Evidence has demonstrated superiority of BCG over transurethral resection of bladder tumor (TURBT) alone or in combination with intravesical chemotherapy. Although a 3-year maintenance protocol is recommended to prevent recurrence in patients with intermediate/high-risk non-muscle-invasive bladder cancer (NMIBC), many patients do not complete the protocol. There are very few studies which have compared the clinical efficacies, optimal dose and toxicity of different BCG strains. The role of performing routine secondary resection (re-TUR) on the survival outcomes is also not clear.
Aim
- This study compared the clinical efficacy of three different BCG strains in patients with intermediate-/high-risk NMIBC and evaluated the importance of performing re-TUR in the setting of BCG maintenance protocol for the three strains.
Method
Study Design
- Retrospective cohort study
Patient Profile
- Intermediate/high-risk BCG-na?ve NMIBC patients who received induction followed by maintenance with 3 BCG strains - Connaught, TICE and RIVM
- Patients treated with the same BCG strain throughout the follow-up.
Treatment Strategy
- The data on patients who underwent re-TUR after primary resection was collected.
- Full BCG therapy comprised induction and 7 maintenance courses.
- Induction was initiated 2-3 weeks after staging TURBT or re-TUR.
- Maintenance protocol was 3 weekly instillations every 3 months for the first 2 courses followed by every 6 months thereafter.
- Cox proportional hazards multivariable regression analysis adjusted for the Spanish Urological Oncology Group (CUETO) prognostic factors, prior recurrence, tumor grade and re-TUR procedures.
Endpoints
- Recurrence-free survival (RFS) defined as months for any stage to relapse
- Progression-free survival (PFS) defined as months for rise to T2 or higher stage
- Cancer-specific survival (CSS)
Results
- Out of the total of 422 patients, 34.6%, 26.5% and 38.7% received Connaught, TICE and RIVM respectively.
- Baseline characteristics were as follows-
- Age, gender and CUETO prognostic risk factors were similar across the groups
- A significant difference in re-TUR was noted among the groups with 30.1%, 48.2% and 56.7% for Connaught, TICE and RIVM respectively.
- 92.9% were high risk, with primary high-grade (HG) Ta-T1 being the most common (69.4%)
- Recurrence rate stratified by re-TUR was 47.9%, 38.4% and 41.5% with Connaught, TICE and RIVM respectively
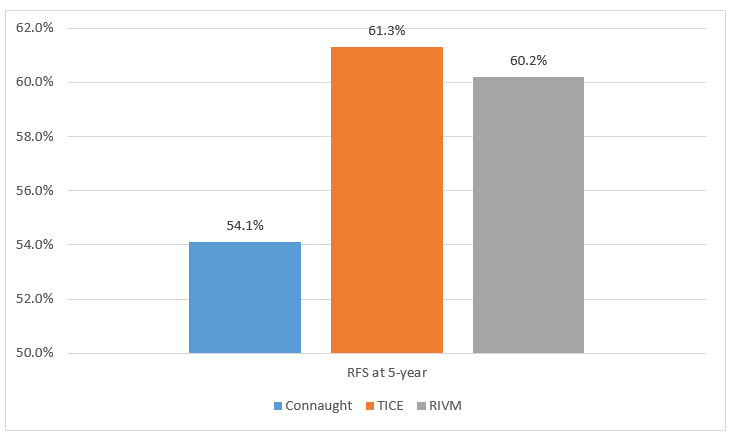
- Comparison of RFS at 5-year among the groups is shown in Figure 1.
Figure 1. Comparison of RFS at 5-year
- Recurrence and progression outcomes were better in patients who had undergone re-TUR (HRRFS: 0.63; HRPFS: 0.55).
- TICE and RIVM had longer RFS as compared to Connaught after adjusting for CUETO risk factors and re-TUR (HRTICE: 0.58; HRRIVM: 0.61).
- There were no significant differences between strains for PFS and CSS.
- In the sub-analysis of only re-TUR patients, TICE was the sole strain to significantly achieve longer RFS compared to both Connaught and RIVM.
- 5-year CSS was 86.7%, 98% and 93.6% for Connaught, TICE and RIVM respectively.
Conclusion
- BCG strains – TICE and RIVM were associated with better recurrence-free survival outcomes as compared to Connaught when administered with a maintenance protocol in intermediate-/high-risk non-muscle invasive bladder cancer patients (NMIBCs).
- The findings confirmed the importance of re-TUR in intermediate-/high-risk NMIBCs and is associated with longer progression-free survival and RFS outcomes.
- TICE had superior RFS outcomes than the other strains after stratifying for re-TUR.
J Cancer Res Clin Oncol. 2021 Oct;147(10):3073-3080. Doi: 10.1007/s00432-021-03571-0.

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


