

Sacubitril/Valsartan Improves Physical and Social Activity Limitations in HFrEF Patients



Background
Heart failure (HF) patients experience a marked reduction in health-related quality of life (HRQL). In fact, such patients have substantial limitations in physical and social activities. The PARADIGM-HF (Prospective Comparison of ARNI With an ACE-Inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure) trial demonstrated improvement in overall HRQL [as determined by the Kansas City Cardiomyopathy Questionnaire (KCCQ)] with sacubitril/valsartan vs. enalapril. This secondary analysis focused on individual physical and social activity items in the KCCQ domains in the PARADIGM-HF trial to enhance the understanding of the responsiveness of each individual activity to sacubitril/valsartan.
Aim
To examine the impact of sacubitril/valsartan on individual physical and social activity in HF patients
Patient Profile
- Patients (age ≥18 years; n=8399) with New York Heart Association (NYHA) class II to IV symptoms having an ejection fraction of ≤40% (changed to ≤35% by protocol amendment) and plasma B-type natriuretic peptide (BNP) ≥150 pg/mL (or N-terminal pro-BNP [NTproBNP] ≥600 pg/mL) or patients hospitalized for HF within last 12 months. (n=8399)
- Patients with lower levels of natriuretic peptides (BNP ≥100 pg/ml or NTproBNP ≥400 pg/ml) were eligible only if they had been hospitalized for HF within 12 months.
- Patients on ongoing therapy were required to tolerate ACE inhibitor or ARB equivalent to at least enalapril 10 mg daily for at least 4 weeks before screening along with stable doses of a ?-blocker (unless contraindicated or not tolerated) and a mineralocorticoid antagonist (if indicated).
Method
Study Design
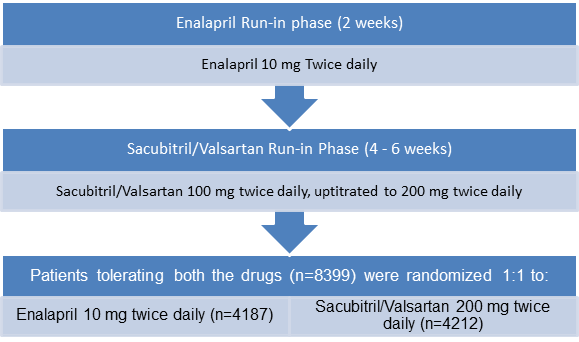
- Multicenter, double-blind, active treatment–controlled, randomized trial with a single-blind run-in period
Treatment Strategy
Assessment of Physical and Social Limitation Attributable to HF
- KCCQ, a disease-specific HRQL questionnaire was administered at baseline and at 4, 8, 12, 24, and 36 months or until final visit. The principal HRQL efficacy time point was pre-specified at 8 months.
Primary Outcome
- Changes in physical and social components of the KCCQ at 8 months and longitudinally
Results
- Of the entire study population, around 90% patients (5987 (78.6%) males and 1631 (21.4%) females) completed the initial KCCQ assessment at baseline (mean age; 64 years)
- At baseline, patients reported greatest limitations for jogging and sexual relationships.
- Adjusted change scores for most physical and social activities at 8 months and during 36 months improved substantially in patients receiving sacubitril/valsartan vs. those receiving enalapril.
- Patients treated with sacubitril/valsartan showed greatest improvements over those treated with enalapril in household chores (adjusted change score difference, 2.35; P < 0.001) and sexual relationships (adjusted change score difference, 2.72; P = 0.002). The benefits persisted through 36 months (overall change score difference, 1.69, P < 0.001; and 2.36, P = 0.001, respectively).
- As per the responder analysis, patients receiving sacubitril/valsartan vs. enalapril had a significant 5-point or greater improvement in change score difference for combined physical and social activity at 8-month follow-up (OR, 1.12; P = 0.04).
- Treatment with sacubitril/ valsartan rather than enalapril was also associated with a significant improvement in walking 100 yards on level ground (OR, 1.13; P = 0.01), gardening (OR, 1.17; P = 0.001), jogging (OR, 1.12; P = 0.02), and hobbies (OR, 1.16; P = 0.002).
- The improvement in combined physical and social activity score at the 8-month visit was comparable to a difference of 9 years of aging (95% CI, 4-13 years) in patients receiving sacubitril/valsartan vs. enalapril.
Conclusions
- In patients with heart failure with reduced ejection fraction, treatment with sacubitril/valsartan rather than enalapril was associated with a significant improvement in nearly all KCCQ physical and social activities. The improvement in scores was most distinct for household chores and sexual relationships.
- Sacubitril/valsartan thus additionally improves limitations in common activities in HFrEF patients while mitigating the risk of CV death, all-cause mortality and HF hospitalization.
Jama Cardiol. April 4, 2018 (Published Online); doi:10.1001/jamacardio.2018.0398.












