

Role of Echocardiographic Biomarkers to Ascertain the Effect of Sacubitril-valsartan on Vascular Properties in Patients with HFrEF



Introduction
Increased vascular stiffness is one of the earliest signs of blood vessel remodeling, and also an independent predictor of mortality in patients with heart failure with reduced ejection fraction (HFrEF). The beneficial impact that sacubitril–valsartan exerts on vascular remodeling through renin–angiotensin–aldosterone system and natriuretic peptide axis may partly contribute towards reduced mortality in HFrEF patients. Till date, echocardiographic biomarkers have not been used to monitor the impact of sacubitril-valsartan on vascular remodeling and function in this patient subgroup.
Aim
To determine whether sacubitril–valsartan therapy would improve aortic distensibility (AD) and fractional area change (AFAC), as assessed by 2D transthoracic echocardiography (TTE) in HFrEF patients over time.
Patient Profile
- Adult patients with congestive HF with New York Heart Association (NYHA) Class II-IV symptoms and with left ventricular ejection fraction (LVEF) ≥ 25% and ≤ 40% (age ≥18 years; n=30)
- All patients were receiving an angiotensin converting enzyme (ACE)-inhibitor or angiotensin receptor blocker (ARB) dose equivalent to enalapril > 10 mg/day, and a beta blocker for at least 4 weeks (unless contraindicated) along with optimal dosing of other HF medications.
- Each patient was initiated on a maximally tolerated dose of sacubitril–valsartan at either 97/103 mg twice daily (n = 22) or 49/51 mg (n = 8).
Methods
Study Design
- Prospective, single-arm cohort study
Assessments
- Serial 2D TTE imaging was performed at baseline, 3 and 6 months following treatment initiation with sacubitril-valsartan.
- Ascending aortic diameters were measured 3 cm above the aortic valve in the parasternal long-axis view and used to calculate AD and AFAC, the markers of vascular compliance.
- AD was defined as the relative cross-sectional diameter change for a given pressure step at a fixed vessel length and AFAC was defined as the percent change of the cross-sectional area (CSA) of the vessel between end-systole and end-diastole
- AD and AFAC was also measured in 30 healthy, age and gender-matched controls at a single time point and used as reference.
Results
- At baseline, individuals in the control group had significantly higher values of AD and AFAC as compared with HFrEF patients (Table 1).
|
Parameter |
Control group |
Sacubitril-valsartan group |
P value |
|
AD |
4.0 cm2dyne−110−3 |
2.2 cm2dyne−110−3 |
< 0.0001 |
|
AFAC |
18.8 % |
10.3 % |
< 0.0001 |
- Treatment with sacubitril–valsartan was associated with a progressive improvement in AD and AFAC from baseline to 6 months in HFrEF patients (Figure 1, Figure 2)
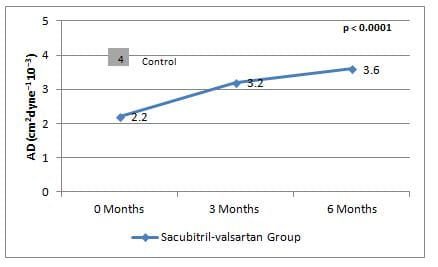
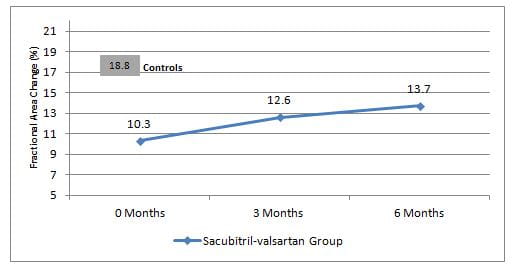
- The significant improvement in AD and AFAC was observed regardless of sacubitril–valsartan dose, and presence/ absence of hypertension, diabetes, or ischemic heart disease
Conclusion
- Treatment with sacubitril–valsartan gradually and progressively improved both AD and AFAC (as measured by TTE) in patients with HFrEF
- Both these echocardiographic markers can be potentially used to assess the effectiveness of sacubitril–valsartan therapy in HFrEF patients.
Int J Cardiovasc Imaging. 2020; 36(2): 271–78.












