

To determine the timing of benefit with intensive statin therapy after an acute coronary syndrome (ACS) in two time windows: an early window soon after an ACS and a late window in more stable patients
PROVE IT-TIMI 22 (Pravastatin or Atorvastatin Evaluation and Infection Therapy: Thrombolysis in Myocardial Infarction-22)

18 Aug, 10


PROVE IT-TIMI 22
Objective
Study Design and Participants
- 4,162 patients who had a total cholesterol level of <240 mg/dl and who had been hospitalized for ACS within the previous 10 days were randomly assigned in a 1:1 ratio to pravastatin 40 mg or atorvastatin 80 mg daily
- Patients were followed up for 18 to 36 months, with an average follow-up of 24 months
Endpoints
- Primary end point was all-cause mortality, myocardial infarction (MI), unstable angina requiring rehospitalization, revascularization (if performed at least 30 days after randomization), and stroke
- Composite triple end point of death, MI, or rehospitalization for recurrent ACS was determined in each group at 30 days
- Composite triple and primary end points were assessed in stable patients from 6 months to the end of study, after censoring for clinical events before 6 months
Results
In comparison to pravastatin, patients receiving atorvastatin showed:
- 15% risk reduction in the primary end point at 15 days
- 28% risk reduction at 30 days in the triple end point
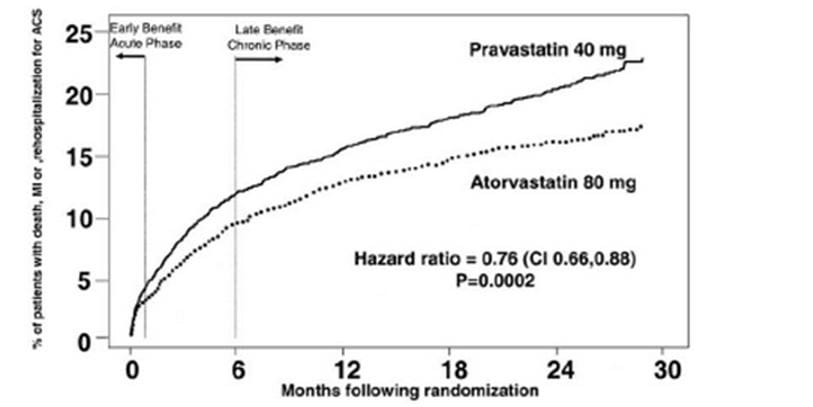
- 15% risk reduction in the primary end point from 6 months to the end of the study
- 28% risk reduction in the triple end point from 6 months to the end of the study
- 24% risk reduction in the overall occurrence of the triple end point
Figure 1. Kaplan-Meier estimates of the composite end point of death, MI, and rehospitalization with recurrent ACS
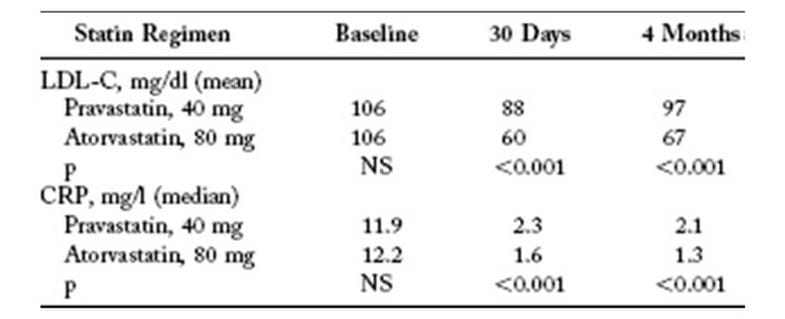
Intensive therapy lowered low-density lipoprotein cholesterol (LDL-C) and C-reactive protein (CRP) more than the standard therapy at 30 days and at four months (Table 1)
Table 1. Effect on LDL-C and CRP
Conclusions
- Intensive versus standard statin therapy leads to a reduction in clinical events within 30 days after an ACS, within a time window consistent with the early pleiotropic effects seen with statins
- Intensive statin therapy provides two windows of cardioprotection in patients with ACS
-
Treatment of patients with ACS should begin in-hospital with high-dose intensive stain therapy to achieve these early clinical benefits and should be continued long-term
J Am Coll Cardiol 2005; 46:1405-10

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26
Journal Scans
25 Jun, 26
25 Jun, 26


