

PROMISE Study: Moxifloxacin, Clinically and Bacteriologically Non-inferior to Ertapenem in Treatment of cIAIs



Introduction
Broad-spectrum antibiotic therapy against both gram-positive and gram-negative microorganisms is essential in the treatment of complicated intra-abdominal infections (cIAIs). Moxifloxacin and ertapenem, both are recommended by the Infectious Diseases Society of America (IDSA) for the treatment of mild-to-moderate community-acquired cIAIs in adults.
Aim
The PROMISE study compared the clinical and bacteriological efficacy and safety of moxifloxacin versus ertapenem for the treatment of cIAIs.
Patients Profile
- N= 804
- Patients with a confirmed or suspected cIAI requiring hospitalisation and i.v. antibiotic therapy (for 5–14 days)
|
Characteristic |
Moxifloxacin |
Ertapenem |
|
|
Age mean ± S.D. (years) |
46.7 (17.8) |
46.1 (17.7) |
|
|
BMI mean ± S.D. (kg/m2) |
26.0 (4.7) |
25.8 (4.6) |
|
|
Initial surgery |
|||
|
Laparotomy [n (%)] |
312 (88.6) |
315 (90.8) |
|
|
Laparoscopy [n (%)] |
40 (11.4) |
31(8.9)c |
|
|
Duration mean ± S.D. (min) |
81.0 (41.5) |
80.8(40.0) |
|
|
Severity of disease at baseline |
|||
|
APACHE II score |
6.9 (4.3) |
6.8(4.6) |
|
|
POSSUM score |
35.3 (7.8) |
34.9 (7.4) |
|
|
Mannheim Peritonitis Index |
19.1 (7.0) |
19.0 (7.3) |
|
|
Origin of infection |
|||
|
Community-acquired [n (%)] |
334 (94.9) |
334 (96.3) |
|
|
Hospital-acquired [n (%)] |
16 (4.5) |
11 (3.2) |
|
|
Primary type of infection [n (%)] |
|||
|
Single abscess |
69 (19.6) |
64 (18.4) |
|
|
Multiple abscesses |
2 (0.6) |
2 (0.6) |
|
|
Localised peritonitis |
100 (28.4) |
96 (27.7) |
|
|
Diffuse peritonitisf |
181 (51.4) |
185 (53.3) |
|
|
Primary cause of infection [n (%)] |
|||
|
Cholecystitis |
33 (9.4) |
32 (9.2) |
|
|
Diverticulitis |
29 (8.2) |
16 (4.6) |
|
|
Trauma |
19 (5.4) |
23 (6.6) |
|
|
Tumour |
13 (3.7) |
13 (3.7) |
|
|
Previous surgery |
15 (4.3) |
9 (2.6) |
|
|
Acute appendicitis |
172 (48.9) |
176 (50.7) |
|
|
Perforated ulcer |
53 (15.1) |
55 (15.9) |
|
|
Other |
18 (5.1) |
23 (6.6) |
|
|
Pre-therapy systemic antibiotic use [n (%)] |
243 (69.0) |
246 |
(70.9) |
S.D., standard deviation; BMI, body mass index; WBC, white blood cell; CRP, C-reactive protein; APACHE, Acute Physiology and Chronic Health Evaluation; POSSUM, Physiological and Operative Severity Score for the Enumeration of Mortality and Morbidity.
Methods
- Randomised, prospective, double-dummy, double-blind, multicentre, non-inferiority study
- 804 patients with cIAIs were randomized to receive either
- Moxifloxacin 400mg (n=410)
- Ertapenem 1g (n= 394)
- Patients were evaluated
- at pre-treatment (within 24 h before initiation of study drug)
- during treatment (daily and complete evaluation on Day 5 ± 1)
- at the end of treatment (EOT) between Day 5 and Day 14
- at the test-of-cure (TOC) visit between 21–28 days after EOT
Study Treatment
- Patients received once-daily i.v. therapy with either 400 mg of moxifloxacin or 1 g of ertapenem in a double-blind manner
- Patients in the moxifloxacin arm received placebo for 30 min immediately followed by moxifloxacin 400 mg in 250 mL over 60 min every 24 h for 5–14 days
- Patients in the ertapenem arm received ertapenem 1.0 g in 50 mL over 30 min followed by placebo for 60 min every 24 h for 5–14 days
Endpoints
- The primary included clinical responses at 21–28 days after the end of treatment (TOC)
- Secondary endpoints included
- Clinical and bacteriological responses at the TOC visit in patients with a bacteriologically documented cIAI
- Bacteriological responses were success (eradication or presumed eradication) or failure (persistence or presumed persistence)
Results
- Moxifloxacin was non-inferior to ertapenem regarding clinical success.
- Bacteriological success rates at TOC with causative organisms were high for both moxifloxacin and ertapenem, respectively
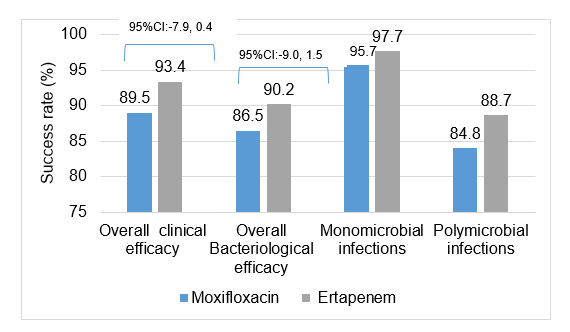
- No significant differences were observed between groups for any of the primary causes or types of cIAI regarding the clinical response.
- There were no major differences between groups regarding the frequency or types of organisms eradicated.
- Clinical success rates were high for both moxifloxacin and ertapenem for each of the five most commonly isolated organisms and across a range of MICs
|
Organism |
Bacteriological success (% of organisms) |
MIC50/90 (mg/L) |
||
|
|
Moxifloxacin |
Ertapenem |
Moxifloxacin |
Ertapenem |
|
Gram-positive aerobes |
83.3 |
88.7 |
|
|
|
Streptococcus anginosus |
81.1 |
89.9 |
0.120/0.250 |
0.120/0.250 |
|
Streptococcus constellatus |
84.3 |
95.2 |
0.120/0.120 |
0.250/0.500 |
|
Gram-negative fermentative rods |
86.4 |
89.6 |
|
|
|
Non-ESBL-producing Escherichia coli |
87.9 |
89.7 |
0.060/0.500 |
≤0.015/≤0.015 |
|
Gram-negative anaerobic rods |
81.8 |
89.6 |
|
|
|
Bacteroides fragilis |
78.9 |
91.6 |
0.500/4.000 |
0.120/0.500 |
|
Bacteroides thetaiotaomicron |
82.2 |
94.4 |
2.000/4.000 |
1.000/1.000 |
- Treatment-emergent adverse events were experienced by >50% of patients in each group, significantly higher with moxifloxacin than ertapenem (P = 0.039)
- The most commonly reported adverse events were wound infections, nausea and increased lipase with both drugs.
- Wound infections (12% versus 7%) and nausea (8% versus 4%) occurred in more moxifloxacin-treated than ertapenem-treated patients
Conclusion
- The PROMISE Study showed that moxifloxacin was clinically and bacteriologically non-inferior to ertapenem in treating cIAIs
- The results indicated that moxifloxacin is a valuable treatment option for a range of community-acquired cIAIs with mild-to-moderate severity when used according to prescribing guidelines
Int J Antimicrob Agents. 2013 Jan;41(1):57-64.












