Multifactorial Intensive Treatment Increases Survival and Time to Incident Cardiovascular Disease in Type-2 Diabetes Patients: Results from the 21-Year Follow-Up of Steno-2 Trial



Introduction
Type-2 diabetes mellitus (T2DM) is a multifactorial disorder with conditions such as hypertension, dyslipidemia and increased platelet aggregation being commonly present in these patients. A multifactorial intensive treatment strategy for the management of T2DM has been shown to result in benefits in terms of increased survival and reduced cardiovascular disease (CVD).
Aim
To determine the long-term impact of ~8 years of intensified multifactorial intervention in patients with T2DM and microalbuminuria in terms of years of life gained and years free from CV event.
Patient Profile
Type-2 diabetes mellitus patients with persistent microalbuminuria (participants of the STENO-2 trial)
Method
Study Design
Observational follow-up of a randomized trial
Treatment Strategies
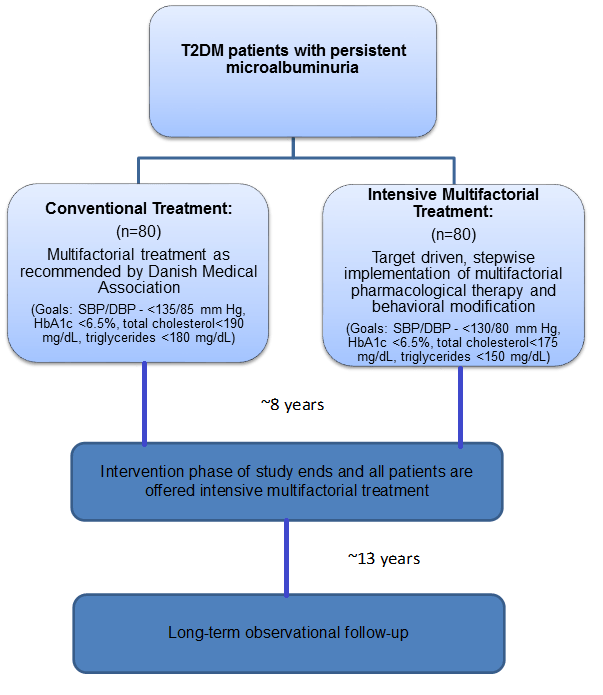
Primary Outcome
- Comparison of the median survival time between the original treatment groups with and without incident CVD, 21.2 years after the initiation of the intervention
Secondary Outcomes
- Composite of CV events (time to incident CVD and number of CV events) as well as mortality and CVD rates.
Tertiary Outcomes
- Rate of incident diabetic nephropathy
- Rate of end stage renal disease (ESRD)
- Development and progression of diabetic retinopathy or neuropathy
Results
- A 45% reduction in all-cause mortality was observed in the original intensive multifactorial treatment group vs. conventional treatment group {Hazard ratio (HR) 0.55; P=0.005}; CV mortality was reduced by 62% in the intensively treated group vs. conventional treatment group (HR 0.38; P= 0.006)
- The patients in the intensive-therapy group had at least 7.9 years longer median survival vs. the patients in the conventional-therapy group
- The median time before first CV event after randomization was 8.1 years longer in the intensive-therapy group
- The risk of all microvascular complications decreased in the intensive-therapy group, except for peripheral neuropathy (Table 1)
|
Complication |
Hazard ratio |
Relative risk reduction |
P value |
|
Retinopathy progression |
0.67 |
33% |
0.005 |
|
Autonomic neuropathy |
0.59 |
41% |
0.011 |
|
Macroalbuminuria |
0.52 |
48% |
0.008 |
|
Peripheral neuropathy |
1.12 |
ND |
0.630 |
ND: no difference
Conclusions
- A 7.8 years of intensified, multifactorial, target-driven treatment in T2DM patients with microalbuminuria was associated with an almost 8 years of longer lifespan over a period of 21.2 years
- Importantly, this increase in lifespan was matched by time free from cardiovascular disease
- Intensive multifactorial treatment must therefore be initiated early in T2DM patients with microalbuminuria to alleviate the CV risk and to improve survival
Diabetologia. 2016; 59: 2298-307