Maintenance and Reliever Therapy with Budesonide/Formoterol Might Reduce the Rate of Severe Exacerbations in Patients with Persistent Asthma



Introduction
The treatment recommended for persistent asthma is a fixed dose inhaled corticosteroid (ICS) or an ICS/long acting ?2-agonist (LABA) combination plus a short acting ?2-agonist (SABA) for relief of symptoms. Despite this, asthma control is still a cause of concern. Latest guidelines recommend the use of budesonide/formoterol as maintenance and reliever therapy (SMART) using one inhaler, without requirement of a separate SABA. The latest Global Initiative for Asthma (GINA) guidelines to recommend this novel approach. Various studies have found SMART therapy effective in reducing the exacerbations. When this study was published, very few had compared the efficacy of SMART therapy with the higher fixed dose of combination therapy.
Aim
To compare the efficacy of budesonide/formoterol for maintenance and relief with salmeterol/fluticasone and a fixed maintenance dose of budesonide/formoterol both with terbutaline for relief in patients with persistent asthma.
Methods
Study design
- Randomized, double-blind trial
- Study comprised of 3 groups who were treated for a period of 24 weeks
- One group of 1123 patients received 2 inhalations of salmeterol/fluticasone 25/125 µg bid plus terbutaline as needed. 1074 completed the study
- Second group of 1105 patients received 1 inhalation of budesonide/formoterol 320/9 µg bid plus terbutaline as needed. 1046 completed the study
- Third group (SMART) of 1107 patients received 1 inhalation of budesonide/formoterol 160/4.5 µg bid plus as needed. 1052 completed the study
Inclusion Criteria
- Patients aged >12 years with asthma for >6 months and using ICS for >3 months
- Forced expiratory volume in 1 sec (FEV1) >50% of predicted normal value with >12% reversibility following terbutaline and >1 asthma exacerbation in previous 12 months
- Patients with reliever medication on >5 of the last 7 days of the 2 week run-in were randomized
- Patients with>10 as-needed inhalations in any day of run-in and who experienced exacerbation during run-in were not randomized
Exclusion Criteria
- Patients using systemic corticosteroids
- Patients with respiratory infections affecting asthma control with 30 days of study entry
Endpoints
Primary endpoint
- Time to first severe exacerbation
Secondary endpoints
- Total number of severe exacerbations
- Total number of inhalations of as-needed medication
- Change in morning and evening peak expiratory flow (PEF)
- FEV1
- Asthma symptom score
- Nights with awakening caused by asthma
- Symptom-free days
- As-needed-free days
- Asthma control days
- Number of mild exacerbations
Results
- The study enrolled 3335 patients
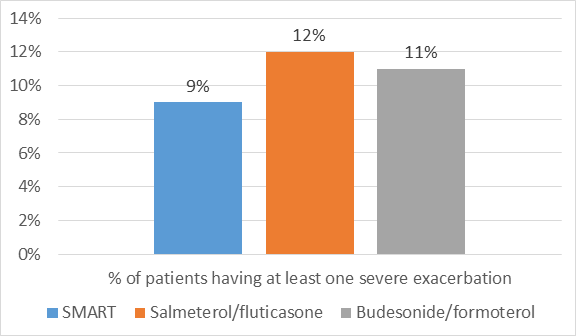
- The time to first severe exacerbation was more prolonged in the SMART group as compared to fixed dose salmeterol/fluticasone and budesonide/formoterol (p=0.0034 and p=0.023 respectively)
- There was 33% reduction in hazard ratio (HR) for a first severe exacerbation with SMART as compared to salmeterol/fluticasone (p=0.003) and 26% reduction as compared to fixed dose budesonide/formoterol (p=0.026) as shown in figure 1.
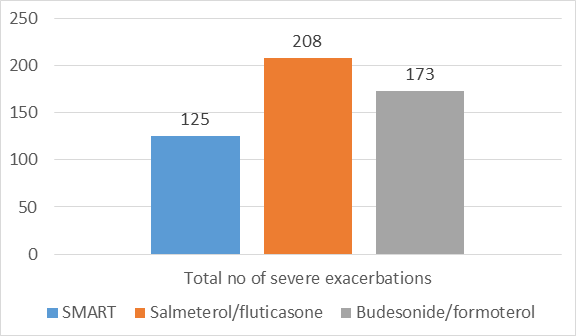
- SMART therapy reduced the total number of severe exacerbations by 39% as compared to salmeterol/fluticasone (p<0.001) and by 28% as compared to fixed dose budesonide/formoterol (p=0.0048) as shown in figure 2.
- The time to first severe exacerbations and the total number of exacerbations were similar in both the fixed dose groups.
- Both the budesonide/formoterol groups had reduced hospitalizations and emergency room treatments as compared to the salmeterol/fluticasone group.
- SMART and budesonide/formoterol groups had 39% and 32% reduction in the total number of hospitalizations (p=0.0015 and p=0.013) respectively.
- The total number of days with exacerbations requiring oral steroids was reduced by 41-45% with SMART as compared to the other 2 groups
- The rates of mild exacerbations were similar among the 3 groups
- The improvement in asthma symptoms and lung function too were similar between all the groups
- As-needed use decreased by 8-9 inhalations per week as compared to baseline in all the 3 groups
- The mean ICS doses were converted to beclomethasone dipropionate (BDP) equivalents based on GINA guidelines
- Compared with fixed-dose budesonide/formoterol treatment, 63% of SMART-treated patients reduced their mean daily dose by at least 160/4.5 µg than 7% who increased their mean daily dose by at least 160/4.5 µg
- There was an overall reduction in the usage of ICS in the SMART group as compared to the other groups
- The overall number of days per treatment group when oral corticosteroids were required was lowest in the SMART group (619 days) as compared to 1044 and 1132 days in the budesonide/formoterol and salmeterol/fluticasone groups respectively
- The safety profile was comparable between the groups
Conclusion
- SMART therapy resulted in a better reduction in the rate of severe asthma exacerbations as compared to twofold higher dose of budesonide/formoterol or a corresponding dose of salmeterol/fluticasone plus SABA
- SMART therapy resulted in a significant improvement over the fixed twice daily combinations of higher dose combination therapy.
- SMART therapy resulted in 50% reduction in the regular maintenance doses of ICS/LABA with improvement in overall asthma control.
Int J Clin Pract. 2007 May 1; 61(5): 725–736. Doi: 10.1111/j.1742-1241.2007.01338.x