Introduction
Elevated blood pressure (BP) and elevated low-density lipoprotein-cholesterol (LDL-C) are both significantly associated with the risk of cardiovascular disease (CVD). Combined lowering/control of both the parameters will therefore substantially alleviate the risk of cardiovascular (CV) events. Majority of CV events occur in individuals without a prior history of CVD, hence a broader population-based intervention to lower BP and LDL would be more effective rather than targeting only the high-risk patients.
Aim
The HOPE (The Heart Outcomes Prevention Evaluation)-3 study was conducted to evaluate the efficacy and safety of a combined LDL cholesterol lowering and BP lowering strategy vs. placebo for preventing major CV events in individuals without CVD but at intermediate-risk.
Patient Profile
- Men (age ≥55 years) and women (age ≥65 years) without CVD, and having at least one CV risk factor (elevated waist-to-hip ratio, history of a low level of high-density lipoprotein cholesterol, current/ recent tobacco use, dysglycemia, family history of premature coronary disease, and mild renal dysfunction)
- Women aged ≥ 60 years with at least 2 of the above CV risk factors
- Around 49.1% of the study population was Asian, 20% subjects were white, 27.5% were Hispanic, and 3.3% were black or belonged to another ethnic group
Methods
Study Design
- A multicenter, long-term, international, double-blind, randomized, placebo-controlled trial with 2-by-2 factorial design
Treatment Strategy
Run-in Phase
- Active BP lowering (fixed combination: candesartan 16 mg/day + hydrochlorothiazide [HCTZ] 12.5 mg/day) and cholesterol lowering (rosuvastatin 10 mg/day) strategy for 4 weeks
- Treatment adherent patients with no unacceptable levels of adverse events (AEs) randomized to one of the following:
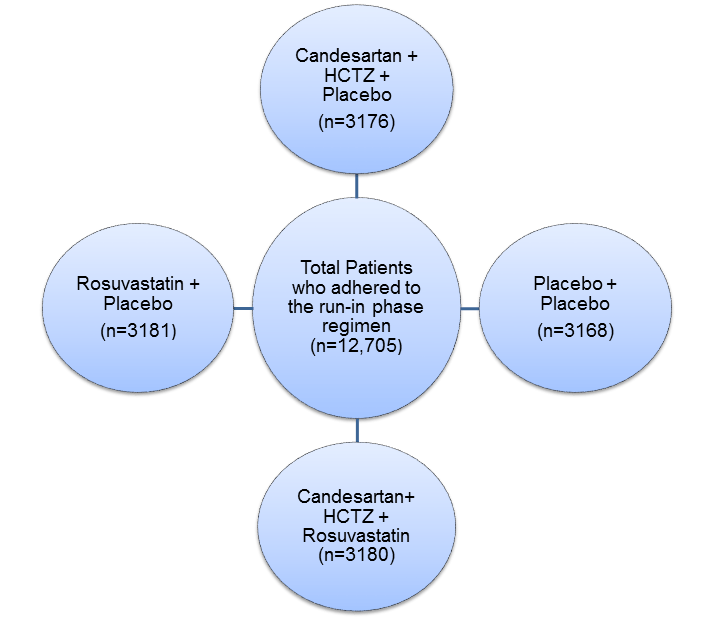
- The present analysis is a comparison of 3180 participants assigned to combined therapy group (with rosuvastatin and two antihypertensive agents) vs. 3168 participants assigned to dual placebo.
Follow-up
- At 6 weeks and 6 months after randomization and every 6 months thereafter
- Median follow-up period: 5.6 years
Primary Outcome
First Coprimary Outcome
- Composite of death from CV causes, nonfatal myocardial infarction, or nonfatal stroke
Second Coprimary Outcome
- Composite of the above events along with resuscitated cardiac arrest, heart failure, or revascularization
Secondary Outcome
- Second coprimary outcome plus angina with evident ischemia
Results
- Systolic BP (SBP) lowered by 6.2 mm Hg, diastolic BP (DBP) by 3.2 mm Hg and LDL cholesterol level by 33.7 mg/dL in the dual therapy group vs. dual placebo group (p <0.001 for all)
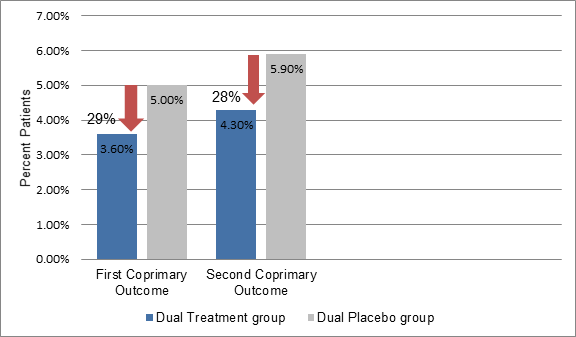
- The incidence of the first coprimary outcome was significantly lower in the combined therapy group vs. the dual placebo group (3.6% vs. 5.0%, hazard ratio [HR]: 0.71, p = 0.005) (29% relative risk reduction [RRR] and 1.4% absolute risk reduction) (Figure 1)
- Similarly, the incidence of the second coprimary outcome was also significantly lower in the combined therapy group vs. the placebo group (4.3% vs. 5.9%, HR: 0.72, p = 0.003, RRR; 28%) (Figure 1)
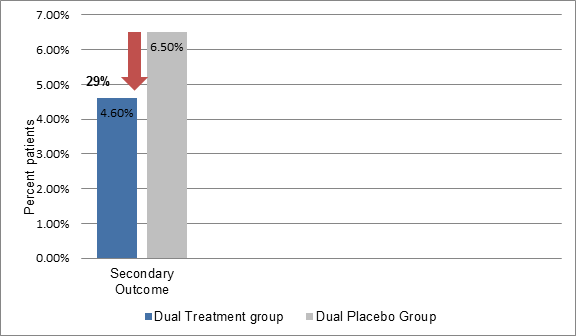
- Fewer subjects in the combined therapy group experienced secondary outcome vs. the dual placebo group (4.6% vs. 6.5%, HR: 0.71, RRR; 29% p=0.001, ) (Table 2)
- Muscle weakness (0.9%) and dizziness (2.2%) were more frequent in the combined therapy group vs. the dual-placebo group. Nevertheless, there were no significant differences for the incidence of new-onset diabetes, renal dysfunction, syncope, liver-function abnormalities, eye problems, or cancers between the study groups
- The overall discontinuation rates were similar in both the study groups
Conclusions
- Fixed doses of rosuvastatin (10 mg/day) and candesartan (16 mg/day) + HCTZ (12.5 mg/day) significantly lowered the risk of CV events as compared to dual placebo during the 5.6 years of treatment in intermediate risk population with average lipid and BP levels but without CVD
- Thus, lowering BP and LDL-C lowered the risk of CV events in intermediate-risk patients without a history of CVD
N Engl J Med 2016; 374(21): 2032-43