

CREDENCE: Impact of Canagliflozin on Cardio-Renal Outcomes in T2DM Patients with CKD



Background
Type-2 diabetes mellitus is one of prime causes of kidney failure globally. Yet, very few effective long-term treatments are available to treat such patients. Currently, renin-angiotensin blockade is the only approved treatment for renoprotection in T2DM patients. Sodium–glucose cotransporter 2 (SGLT2) inhibitors that lower blood glucose levels, have shown reduction in cardiovascular (CV) events in several trials. Secondary analyses of these trials have also hinted on improved renal outcomes in T2DM patients treated with SGLT2 inhibitors, but the evidence with this respect is discrepant.
Aim
CREDENCE (Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation) trial assessed the impact of canagliflozin (an SGLT2 inhibitor) on cardio-renal outcomes in T2DM patients with co-existing albuminuric chronic kidney disease (CKD).
Patient Profile
- Type-2 diabetes patients with glycated hemoglobin (HbA1c) 6.5%-12% (age ≥30 years, n=4401)
- All patients had albuminuric CKD (an estimated glomerular filtration rate [eGFR] 30 to <90 ml/min/1.73 m2 of body-surface area and albuminuria (urinary albumin-to-creatinine ratio, >300 to 5000; albumin measured in milligrams and creatinine in grams)
- All the patients received a stable dose of an angiotensin-converting–enzyme inhibitor (ACEI) or angiotensin-receptor blocker (ARB) for at least 4 weeks before randomization. Dual-agent treatment with an ACEI and an ARB, a direct renin inhibitor, or a mineralocorticoid-receptor antagonist was not allowed.
Methods
Study Design
- Double-blind, randomized placebo-controlled, multicenter (conducted across 690 site in 34 countries) clinical trial
Treatment Strategy
- Patients were randomized as follows:
Follow-Up
- Median follow-up period: 2.62 years
- Follow-up visits were conducted at weeks 3, 13 and 26; post-randomization. This was followed by alternate telephone calls and clinic visits at 13-week interval.
- Patients’ feet were also examined at each follow-up visit to assess the risk of limb amputation. The treatment was temporarily discontinued in case of active condition that could result in amputation.
Outcomes
Primary Outcome
- A composite of end-stage renal disease (ESRD; dialysis, transplantation, or a sustained eGFR of <15 ml/min/1.73 m2), a doubling of the serum creatinine level, or death from renal or CV causes
Prespecified Secondary Outcomes
- A composite of CV death or hospitalization for heart failure (HF)
- A composite of CV death, myocardial infarction (MI), or stroke
- Hospitalization for HF
- A composite of ESRD, doubling of the serum creatinine level, or renal death
- CV death
- Death from any cause
- A composite of CV death, MI, stroke, or hospitalization for HF or for unstable angina
Safety Outcomes
- Incidence of fractures, pancreatitis, ketoacidosis, and renal-cell carcinoma
Results
- The trial was terminated early after a planned interim analysis on the recommendation of the data and safety monitoring committee as clinical benefits were evident well before the trial completion.
- Mean age of the study population was 63 years and 33.9% were females. Mean HbA1c of the study population was 8.3%, mean eGFR was 56.2 ml/min/1.732 and median urinary albumin-to-creatinine ratio was 927 mg/g.
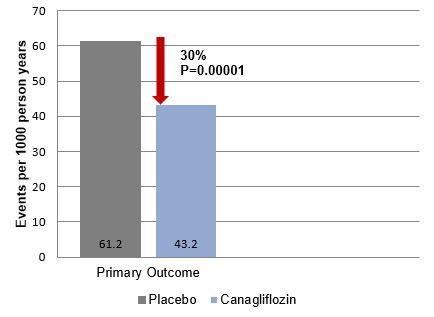
- Patients treated with canagliflozin had a 30% relative risk reduction (RRR) for the primary outcome as compared to those treated with placebo, with event rates of 43.2 and 61.2 per 1000 patient-years, respectively (hazard ratio [HR], 0.70; 95% confidence interval [CI], 0.59 to 0.82; P = 0.00001) (Figure 1).
- Patients treated with canagliflozin had a 34% RRR for the renal-specific composite of ESRD, a doubling of the creatinine level, or death from renal causes was (HR, 0.66; 95% CI, 0.53 to 0.81; P<0.001), and 32% RRR for ESRD (HR, 0.68; 95% CI, 0.54 to 0.86; P = 0.002).
- Patients treated with canagliflozin also had a 20% lower risk of CV death, MI, or stroke (HR, 0.80; 95% CI, 0.67 to 0.95; P = 0.01) and 39% lower risk of hospitalization for HF (HR, 0.61; 95% CI, 0.47 to 0.80; P<0.001).
- An increased risk of lower limb amputation was identified in another trial of canagliflozin. As a result, the incidence of amputation was recorded for CREDENCE as well. Rates of amputation (12.3 versus 11.2 per 1000 patient-years, HR; 1.11, 95% CI, 0.79 to 1.56) or fracture (HR; 0.98; 95% CI, 0.70 to 1.37) did not differ significantly in the canagliflozin and placebo treated subjects. Overall, the incidence of ketoacidosis was low but higher in canagliflozin-treated patients vs. placebo-treated patients (2.2 vs. 0.2 per 1000 patient-years).
- The overall mean difference in the HbA1c reduction between canagliflozin and placebo throughout the trial was 0.25%.
- A greater reduction in the eGFR was observed in the canagliflozin group vs. the placebo group during the first three weeks (–3.72 vs. –0.55 ml/min/1.73 m2, between-group difference of –3.17 ml/min/1.73 m2 (95% CI, –3.87 to –2.47). Thereafter, the decline in the eGFR was slower in the canagliflozin group vs. the placebo group (–1.85 vs.–4.59 ml/min/1.73 m2/year; between–group difference; 2.74 ml/min/1.73 m2/year).
Conclusions
- Canagliflozin treatment was associated with a lower risk of kidney disease, risk of kidney failure and CV events vs. placebo in T2DM patients with CKD at a median follow-up of 2.62 years.
- Canagliflozin-treated patients also had a lower risk of ESRD, hospitalization for HF, and the composite of CV death, MI, or stroke.
- Canagliflozin may effectively render renal and CV protection in T2DM patients with CKD.
N Engl J Med. 2019; 380 (24): 2295-306.












