

CGM may Improve the Glycemic Control in T2DM Patients Treated with Basal Insulin

15 Jun, 21


Introduction
Continuous glucose monitoring (CGM) is associated with improved glycemic control in type-2 diabetes mellitus (T2DM) patients treated with intensive insulin therapy. However, little is known about the role of CGM in T2DM patients treated with basal insulin without prandial insulin (less intensive treatment).
Aim
To determine the effectiveness of CGM in adult T2DM patients treated with basal insulin without prandial insulin
Patient Profile
- Adult T2DM patients (age ≥30 years) treated with 1 or 2 daily injections of long- or intermediate-acting basal insulin for at least 6 months, without prandial insulin, with or without noninsulin glucose-lowering medications, with glycosylated hemoglobin (HbA1c): 7.8%–11.5% and self-reported blood glucose monitoring (BGM) testing averaging ≥3 times per week
Methods
Study Design
- A randomized, multicentre, open-label, parallel group trial, conducted across 15 centers in the US
Interventions
- The study participants were randomized 2:1 to CGM (n = 116) or traditional blood glucose meter (BGM) monitoring (n = 59)
Outcomes
Primary Outcome
- HbA1c level at 8 months
Secondary Outcomes
- CGM-measured time in target glucose range of 70–180mg/dL
- Time with glucose level >250mg/dL
- Mean glucose level at 8 months
Exploratory Outcomes
- Time at >180 mg/dL
- Time at <70 mg/dL
- Time at <54 mg/dL
Follow-up Visits
- At 2 weeks, and at 1 and 8 months
- Telephonic follow-up after 2, 4 and 6 months
Results
- The mean age of the study population was 57 years, 88 of them were women and the mean baseline HbA1c level was 9.1%. Of the study participants, 165 (94%) completed the study.
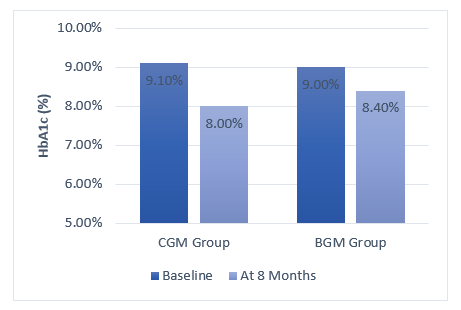
- Patients in the CGM group had a significantly greater decrease in mean HbA1c level from baseline to 8 months (9.1% to 8.0% vs. 9.0% to 8.4%; adjusted difference, −0.4%; P = 0.02) (Fig 1).
Fig 1: Decrease in the HbA1c levels during the study
- At 8 months, the time in the target glucose range of 70 to 180mg/dL was higher for the patients in the CGM group vs. those in the BGM group. Conversely; the mean percentage of time at >250 mg/dL was lower for the patients in the CGM group vs. the BGM group. Patients in the CGM group also had lower mean glucose values at 8 months as compared with those in the BGM group. (Table 1).
Table 1: Secondary outcomes during the study
|
Outcome |
CGM Group |
BGM Group |
Adjusted Difference |
P value |
|
% Time in range of 70-180 mg/dL |
59% |
43% |
15% |
< 0.001 |
|
% Time >250 mg/dL |
11% |
27% |
-16% |
<0.001 |
|
Mean Glucose Values |
179 mg/dL |
206 mg/dL |
-26 mg/dL |
<0.001 |
- The exploratory analysis indicated a reduction in CGM-measured hypoglycemia in the CGM vs. the BGM group at 8 months for time at less than 54 mg/dL (adjusted mean difference, −0.10%; P = 0.001) and time at less than 70 mg/dL (adjusted mean difference, −0.24%; P = 0.02).
- The incidence of severe hypoglycemia in CGM group was 1% and that in BGM group was 2%.
- Amongst the patients in the CGM group, the mean score on the CGM satisfaction scale was 4.1 with mean scores of 4.2 on the benefits subscale and 1.9 on the hassles subscale. A higher score on the benefit subscale and a lower score on the hassles subscale indicates greater value of CGM.
Conclusions
- Amongst adult T2DM patients with poor glycemic control who were treated with basal insulin without prandial insulin, use of CGM was associated with significantly lower HbA1c levels at 8 months as compared with the use of BGM monitoring.
JAMA. June 2, 2021 (Published Online); doi:10.1001/jama.2021.7444.

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


