AVICA: A Head-to-Head Comparison of Acetaminophen vs. Ibuprofen in Young Children with Mild Persistent Asthma



Introduction
Studies in past have indicated a link between frequent acetaminophen use and asthma-related complications among children. Consequently, some physicians do not recommend acetaminophen in children with asthma. Nevertheless, this issue has not been investigated with appropriately designed trials.
Aim
The Acetaminophen versus Ibuprofen in Children with Asthma (AVICA) trial was initiated to determine whether the use of acetaminophen vs. ibuprofen under clinical indication would result in higher morbidity related to asthma in children with mild persistent asthma.
Patient Profile
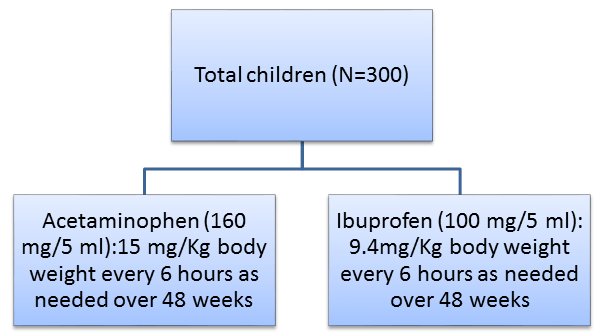
- Children with mild persistent asthma (age group, 12 to 59 months; n=300)
Methods
Study Design
- A multicenter, randomized, double-blind, parallel trial
Run-in-period
- 2 to 8 weeks prior to randomization
Treatment Strategy
- All participants were already receiving standardized asthma-controller therapies as used in the Individualized Therapy for Asthma in Toddlers (INFANT) trial:
- Daily use of inhaled glucocorticoids (fluticasone propionate, two inhalations at 44 ?g each, twice daily)
- Daily use of an oral leukotriene-receptor antagonist (montelukast, 4 mg, once daily at bedtime)
- Use of inhaled glucocorticoids, as-needed (fluticasone propionate, two inhalations at
- 44 ?g each, with each use of open-label albuterol sulfate)
- Patients received the assigned analgesic on an as-needed basis (for the alleviation of fever or pain) over the course of the 48 weeks
Follow-Up
- 48 weeks
Primary Outcome
- The number of asthma exacerbations that led to treatment with systemic glucocorticoids
Secondary Outcomes
- The percentage of asthma-control days
- The average use of rescue albuterol
- The frequency of unscheduled health care utilization for asthma
Results
- Study subjects received a median of 5.5 doses of trial medication; with no significant between-group difference in the median number of doses received (P = 0.47).
- The number of asthma exacerbations for acetaminophen vs. ibuprofen group (0.81 vs. 0.87 per participant) did not differ significantly during the 46 weeks of follow-up (relative rate of asthma exacerbations in the acetaminophen group vs. the ibuprofen group, 0.94; P = 0.67).
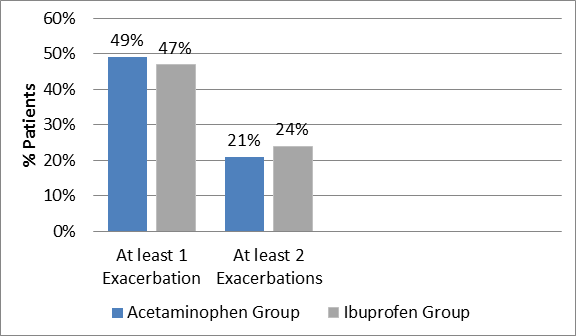
- Nearly 49% of the children on acetaminophen experienced at least one asthma exacerbation and 21% had at least two such events. Similarly, 47% and 24%, of children administering ibuprofen had at least one or two asthma exacerbations, respectively (Figure 1)
- The percentage of asthma-control days, use of an albuterol rescue inhaler and unscheduled health care utilization for asthma did not differ amongst the acetaminophen and ibuprofen users (Table 1).
|
Outcome |
Acetaminophen Group |
Ibuprofen Group |
P value |
|
% of asthma-control days |
85.8% |
86.8% |
0.50 |
|
Use of an albuterol rescue inhaler |
2.8 inhalations per week |
3.0 inhalations per week |
0.69 |
|
Unscheduled health care utilization for asthma |
0.75 episodes per participant |
0.76 episodes per participant |
0.94 |
Conclusion
- As-needed use of acetaminophen among young children with mild persistent asthma did not increase the incidence of asthma exacerbations or asthma-related complications as compared to the as-needed use of ibuprofen.
New Engl J Med. 2016; 375: 619-30