Speaker: Dr. Mario I. Fernández, Chile
Important Takeaways
-
BCG is still the first-line treatment for high-risk bladder cancer, recommended for 1-3 years with maintenance therapy.
-
Vaccinated or previously exposed patients show lower recurrence rates, suggesting potential benefits from immunisation.
-
Intravesical gemcitabine-docetaxel (gem/doce) offers promising outcomes, with early trials reporting high recurrence-free survival rates at 2 years.
-
Ongoing trials (BRIDGE trial) are comparing gem/do with BCG to determine whether it can become a viable alternative with fewer side effects.
-
Checkpoint inhibitor trials (like POAC, ALBAN, KEN 6667) are exploring systemic immunotherapies in BCG-naive settings.
-
The TAR-200 device, combined with checkpoint inhibitors or as monotherapy, is being evaluated in new clinical trials.
-
Gem/Doce therapy is well tolerated, offering better quality of life compared to BCG, with fewer urinary side effects.
Key Highlights
BCG as First-Line Standard:
BCG remains the primary treatment for high-risk NMIBC, with guidelines from the European Association of Urology (EAU) and the American Urological Association (AUA) recommending one to three years of full-dose maintenance following induction.
Proper administration with an optimal maintenance schedule is crucial for maximising BCG’s efficacy, with the SWOG regimen (developed by Dr. Donald Lamm) cited as the benchmark for robust outcomes in high-risk patients.
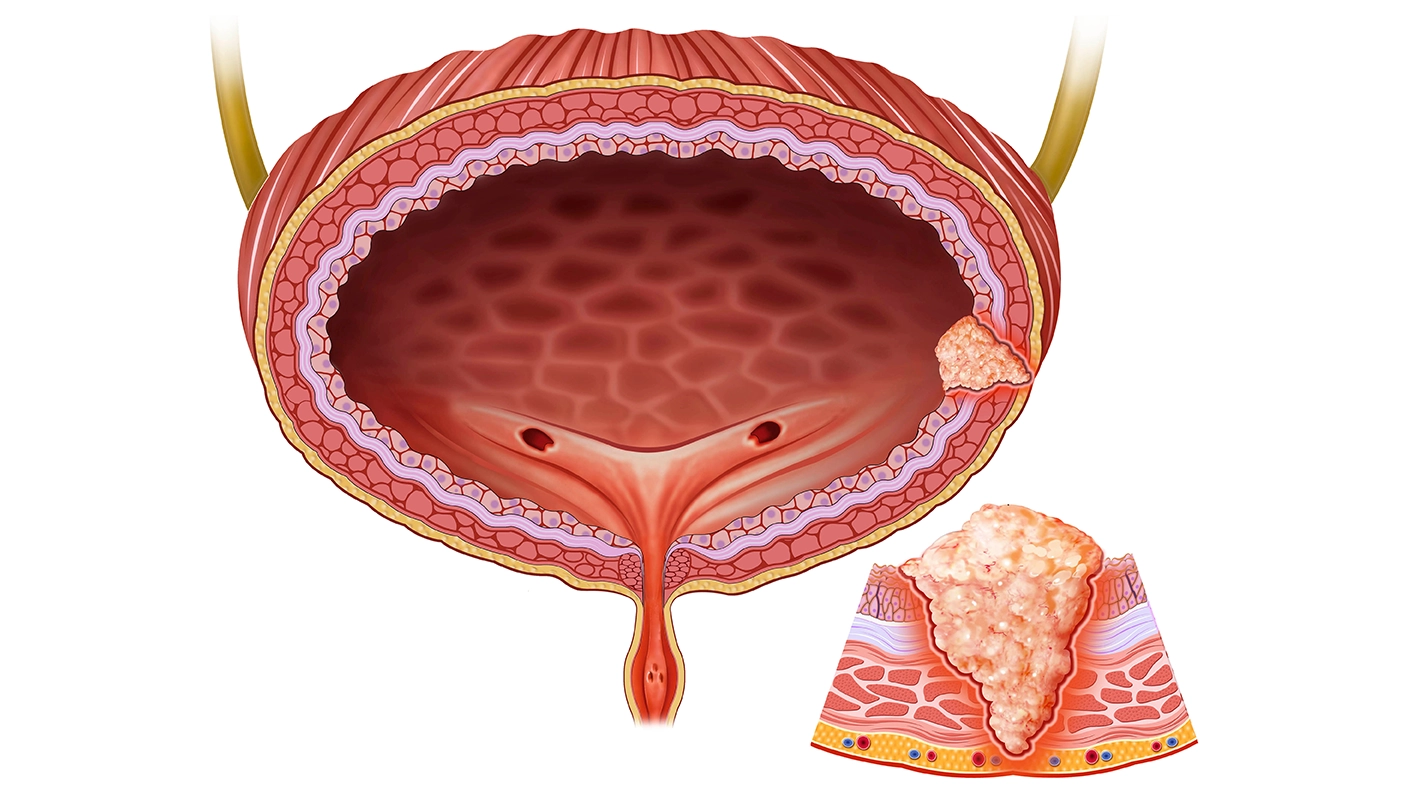
Real-World Efficacy of BCG in High-Risk Patients:
Data from MD Anderson Cancer Center and the speaker’s institution in Tel Aviv demonstrate improved outcomes when BCG is administered according to optimal protocols, showing a one-year recurrence rate of just 10% to 19% and five-year progression rates as low as 2% to 8%. These results underscore that BCG remains highly effective for high-risk patients when given under ideal conditions, yet persistent challenges with global BCG shortages necessitate exploring other viable strategies.
Mitigating BCG Shortages:
Strategies for overcoming BCG shortages include reducing maintenance duration to one year and using dose reductions (e.g., one-third dose). A systematic review of studies, including controlled trials, showed that full-dose BCG may offer a slight advantage over reduced doses, but one-third dosing with one-year maintenance remains an effective alternative in shortage situations.
Emerging Treatment Options:
Intravesical Gemcitabine and Docetaxel (Gem/Doce): Gem/Doce has shown promise as a viable alternative to BCG, especially for BCG-unresponsive NMIBC. Data from the University of Iowa indicate a two-year recurrence-free survival of up to 90%, with no progression or cancer-specific mortality reported in this high-risk group. The BRIDGE trial is currently underway in the U.S., comparing standard BCG therapy with Gem/Doce for up to three years. If Gem/Doce proves non-inferior to BCG, it could become a frontline treatment option, especially for patients experiencing BCG toxicity.
Systemic Immunotherapy with Checkpoint Inhibitors:
Trials are investigating the use of checkpoint inhibitors (e.g., pembrolizumab) combined with BCG or as monotherapy. Four active trials (POTOMAC, ALBAN, CREST, and KEYNOTE-676) are exploring checkpoint inhibitors in high-risk NMIBC, with results expected in about three years.
Novel Delivery Systems: TAR-200 Device:
The TAR-200 device, an intravesical release system for gemcitabine, is being evaluated as a combination therapy with checkpoint inhibitors in the BCG-naïve setting under the SUNRISE-3 trial. This system offers controlled drug release within the bladder, potentially improving drug efficacy and reducing the need for frequent instillations.
Future Directions and Clinical Trials:
Ongoing trials, including the SWOG 1602 (examining strain-specific BCG efficacy) and studies evaluating pretreatment BCG vaccination, will likely clarify the roles of different strains and potential immunologic priming methods.
Results from the BRIDGE and SUNRISE-3 trials, among others, are anticipated to define the comparative efficacy and safety of Gem/Doce, TAR-200, and immunotherapies in the BCG-naïve setting.
Dr. Fernandez underscored the importance of adhering to established BCG protocols while also embracing the expanding treatment landscape for NMIBC, ensuring that patients receive the most effective and personalised care possible.
Société Internationale d'Urologie Congress, 23-26 October 2024, New Delhi, India.