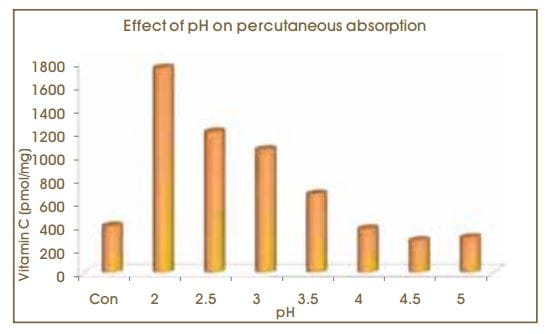
The 15% formulations of L-ascorbic acid were tested at pH levels between 2 and 5. Tissue levels of L-ascorbic
acid were enhanced only at a formulation with pH levels less than 3.5. Thus L-ascorbic acid must be
formulated at pH levels less than 3.5 to enter into the skin.
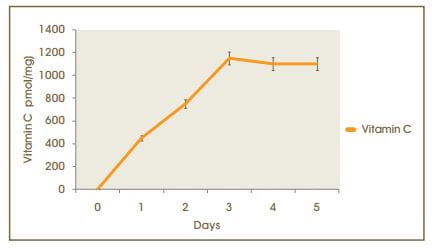
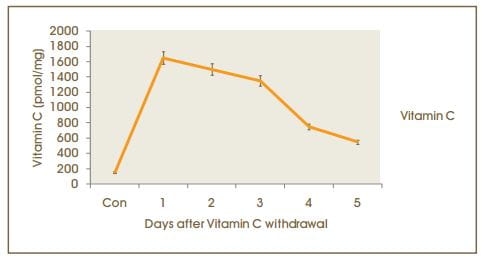
After 5 days of 15% of L-ascorbic acid applications skin levels were measured at daily intervals with no
further topical applications. The half-life of L-ascorbic acid in tissue was found to be approximately 4
days.
Figure. 5: Washout of skin L- ascorbic acid
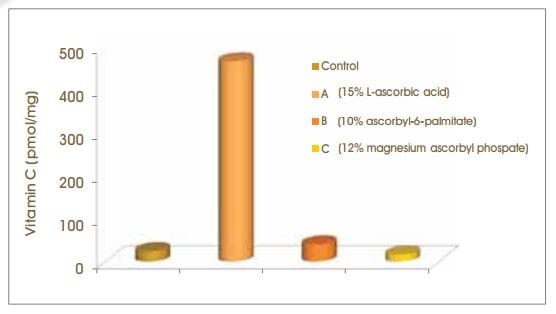
Because it is difficult to formulate a stable form of L-ascorbic acid more stable derivatives like
magnesium ascorbyl phosphate and ascorbyl-6-palmitate have been utilized in the topical formulation.
Accordingly 15% L-ascorbic acid
Figure.6: Percutaneous absorption of ascorbic acid derivatives
Topical absorption has been proved by radioactive labelling studies in pigs.
After treatment with 10% vitamin C cream, 8.2% was found in the dermis and 0.7% was in the
blood.7
So, topical L-ascorbic acid provides a safe and effective supplement to normal tissue stores. It must
be formulated at high concentrations and at a pH lower than 3.5 to be effective.
Use of topical ascorbic acid and its effect on photodamaged skin topography
In a 3-month randomized, double-blind, vehicle-controlled study, 19 patients with mild to moderate
photodamaged skin were enrolled. Coded and unmarked medications were randomly assigned to the left
and right sides of each subject's face - one containing the topical vitamin C (L-ascorbic acid)
and the other, the vehicle serum. Three drops (0.5 ml) of each formulation were applied daily to the
randomly assigned hemi-faces over the 3-month study period.
Figure. 7: Clinical investigator's assessment
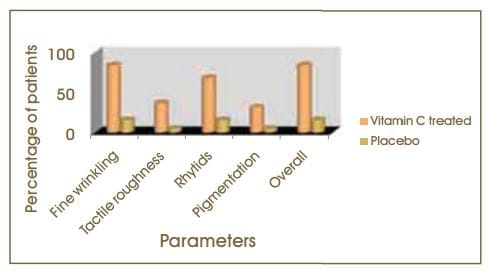
Clinical assessment demonstrated a statistically significant improvement with active treat ment
greater than the control for fine wrinkling tactile roughness coarse rhytides skin laxity/tone
shallowness/yellowing and overall features. Altogether 84.2% of vitamin.
Figure. 8: Subject self - appraisal of overall improvement
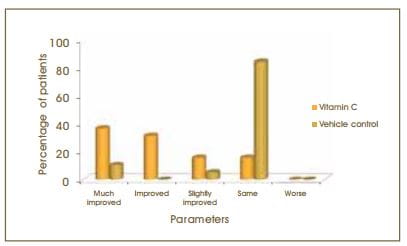
The above graph summarizes the patient questionnaire results. The active side was preferred over the
control side by 84.2% of the subjects. Photographic assessment showed that the active treatment was
preferred over the control side by 57.9% of patients.
Conclusion
This 3-month study demonstrated a topographic improvement in photodamaged facial skin treated with
topical Vitamin C (L-ascorbic acid).
Double-Blind, Half-Face Study Comparing Topical Vitamin C and Vehicle for Rejuvenation of
Photodamage13
In a double-blind, 90-day pilot study, 10 patients having tacial photodamage were recruited. The
active vitamin C (L-ascorbic acid) complex was applied to one side of the face and the inactive
placebo base was applied to the opposite side of the face once a day.
Clincial evaluation of wrinkling, pigmentation, inflammation, and hydration was per -formed prior to
the study and at weeks 4, 8, and 12. At 12 weeks, 2 mm punch biopsies of the lateral cheeks were
performed in 4 patients and stained with haematoxylin and eosin; in situ hybridization studies were
also conducted using an anti-sense probe for mRNA for type I collagen. A questionnaire was also
completed by each patient.
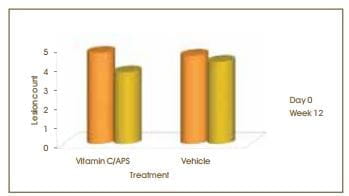
Table 1: Topical vitamin C: Average improvement in wrinkle scores
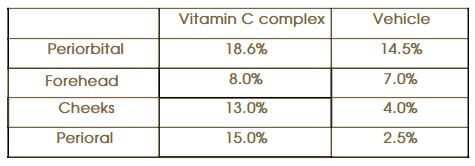
At the end of the study, when the two sides were compared statistically, a significant difference in
the clinical scoring of facial wrinkles was detected in the perioral and cheek areas of the 10
patients.
There was also statistically significant improvement of the entire treated side, compared to its
beginning point, and no significant change on the base side.
Biopsies of treated versus untreated areas confirmed the presence of increased amounts of collagen in
those patients showing clinical improvement. No patients were found to have any evidence of
inflammation. Hydration was improved bilaterally. While 4 patients felt that the vitamin C-treated
side had improved unilaterally, no patient felt that the placebo side showed unilateral improvement.
Conclusion
This pilot study demonstrated that a properly formulated vitamin C topical product may play a
significant role in the reversal of photodamage of the skin. This type of product may be used as
part of an overall programme using other topical agents, with or without other procedures such as
various ablative and non-ablative laser therapies, acid peel resurfacing or dermabrasion.
A double-blind randomized trial of 5% ascorbic acid vs 4% hydroquinone in melasma10
In a randomized, double-blind comparative study, 16 female patients with a pair of bilaterally
symmetrical lesions of melasma were enrolled. Their ages ranged from 23 to 43 years. While 8
patients had the epidermal type of lesions, another 8 had the mixed type. The patients were randomly
assigned in a double-blind manner to apply, on the left or right side of the face, 5% vitamin C
(L-ascorbic acid) or 4% hydroquinone water-oil emulsion. All the patients were supervised every 4
weeks during a 16-week period.
Colorimetric assessment was calculated by obtaining the melanin index difference between the targeted
lesion and pre-lesion areas. This was performed initially and at the end of the study. There was no
difference found between the two sides (p=0.052). The lightening effect of hydroquinone was evident
as early as the first month of treatment, whereas that of vitamin C (L-ascorbic acid) was noted at
the third month.
Figure. 9: Subjective improvement
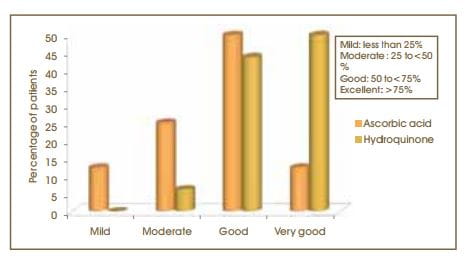
As per the subjective assessment by patients, 93% of patients had good (50- 75%) to excellent
(>75%) improvement with hydroquinone, compared to 62.5% with topical vitamin C (L-ascorbic acid).
A similar number of patients felt a 50- 75% improvement with both treatments.
With regard to adverse effects, 1 patient experienced irritation with vitamin C (L-ascorbic acid)
(6.25%) and 11 patients with hydroquinone (68.75%)
Conclusion
Vitamin C (L-ascorbic acid) has a beneficial effect on melasma, with a minimum of adverse effects.
Vitamin C (L-ascorbic acid) can be used for a longer period of time as part of the initial hyper
pigmentation treatment and as a maintenance therapy.
Sodium L-ascorbyl-2-phosphate 5% lotion for the treatment ofocne vulgaris; a randomized
double-blind controlled trial14
Figure. 10: Investigator's Global Assessment
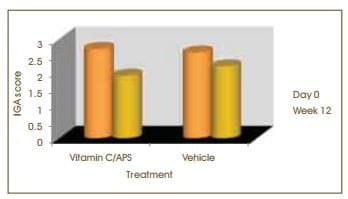
By 12 weeks of treatment 61 % of subjects showed improvement in acne compared to only 38% of patients
with placebo
Figure. 11: Subject's Global Assessment Score
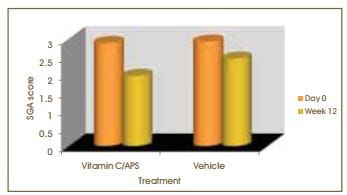
As per the SGA 71 % of subjects showed improvement in acne by 12 weeks of therapy compared to 52%
with placebo.
Figure. 12: Inflammatory lesion count
Vitamin C demonstrated a statistically significant decrease in inflammatory acne lesions.
Conclusion
This study demonstrates that 5% sodium L-ascorbyl-2-phosphate is efficacious as monotherapy for the
treatment of acne. This therapy demonstrated minimal irritation.
APS may offer an ideal adjunct therapy to common acne regimens.
Open study comparing 5% Sodium L- ascorbyl 2- phosphate iotion versus 1% clindamycin phosphate iotion
for acne vulgaris 15
In a multicentre, open-label study, 70 patients with at least ten and fewer than fifty inflammatory
lesions, at least ten and fewer than hundred non-inflammatory lesions and no more than two
nodulocystic lesions on the face were enrolled.
Enrolled patients were randomized to apply either 5% sodium L-ascorbyl-2- phosphate (APS) lotion or 1
% clindamycin phosphate lotion (CL) in the morning and in the evening for 12 consecutive weeks.
Figure. 13: Percentage of patients with good and excellent improvement scores
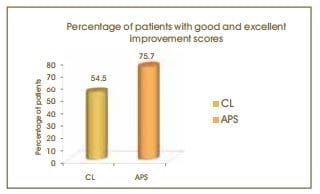
75.7% of patients in the APS treatment group showed either good or excellent improvement compared to
54.5% in the CL treatment group
Figure. 14: Mean percentage reduction of inflammatory and non-inflammatory lesions after 12 weeks of
treatment
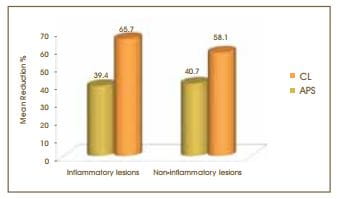
Mean percentage reductions in the inflammatory and non-intlammatory lesion counts were statistically
significant in the APS treatment group compared with the CL group.
Study results demonstrated the superiority of APS over CL in the treatment of facial acne. APS was
shown to be superior to CL in percentage reduction in inflammatory and noninflammatory lesions, as
well as the global improvement scores.
Conclusion
APS was found to be more efficacious than CL in the treatment of facial acne vulgaris.
Comparison of clinical efficacies of sodium ascorbyl phosphate, retinol and their combination in
acne treatment 16
In this cross, double- blind study, 30 subjects having facial acne of grade ll-lll, with ten to fifty
inflammatory lesions were included in the study. The subjects were randomly assigned to use 5%
sodium ascorbyl phosphate (SAP) with a control base cream, 0.25 retinol cream with a control base
lotion, and 5% SAP lotion along with 0.2% retinol separately.
Subjects using retinol cream were advised to use it during the night time for the same period.
For the combination treatment group, subjects were assigned 5% SAP lotion twice daily and 0.2%
retinol cream once daily.
Figure. 15: Percentage reduction of lesions in each treatment group

Acne vulgaris treated with 5% SAP was not significantly different from that of 0.2% retinol at
baseline following 4 to 8 weeks of application.
The combination treatment significantly reduced inflammatory lesions, compared with 5% SAP and 0.2%
retinol following 8 weeks of treatment.
Conclusion
The combination treatment of 5% SAP and 0.2% retinol was most effective in reducing inflammatory
lesions because it incorporated the synergistic effects on lipid peroxidation and the sebaceous
glands function, in addition to the enhancement of SAP permeability by the desquamation of the
stratum corneum influenced by retinol, keratin plug removal and the anti-inflammatory effect of
retinol. The synergistic effect of these two active ingredients results in a potent remedy for acne
vulgaris.
Effect of vitamin C on postoperative C02 laser resurfacing erythema 9
Post-operative erythema of several months duration is a universal and problematic side effect of
cutaneous carbon dioxide (C02) laser resurfacing. The following study was conducted to determine the
effectiveness of two formulations of topical vitamin C (L-ascorbic acid) in reducing the degree and
duration of erythema post-C02, laser resurfacing.
At 13 to 42 days post-operatively (mean: 23.5 days) one-half of each patient's face was randomly
selected for application of topical vitamin C (L-ascorbic acid) serum (11 patients) or cream (10
patients) once daily for a period of 8 weeks. Patients applied a bland emollient on the control
side.
In each group 8 out of 10 patients displayed a greater reduction in erythema with topical vitamin C
(L-ascorbic acid), compared with the control half.
The average difference in the erythema readings at baseline, compared with those obtained at week 8,
was 3.86 for the facial half treated with vitamin C (L-ascorbic acid) cream and 2.53 for the control
facial half. Similarly these readings were 3.06 and 2.56 with vitamin C (L-ascorbic acid) serum and
control, respectively.
Figure. 16: Decrease in erythema
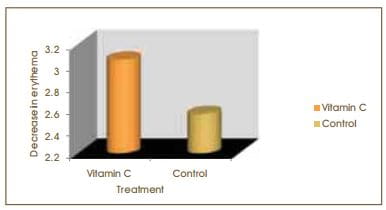
Application of vitamin C (L-ascorbic acid) results in a more rapid resolution of erythema, compared
to bland emollient, when topical therapy is initiated 2 or more weeks after laser resurfacing
procedure.
Conclusion
Topical vitamin C (L-ascorbic acid), when used in an appropriate vehicle and when initiated 2 or more
weeks post-operatively, may decrease the degree and duration of erythema after cutaneous C02 laser
resurfacing.
VC 15 is the first vitamin C serum in India.lt contains L-ascorbic acid at a concentration of 15%. It
is a stable formulation with a pH of 2.7. VC 15 promises to be non-irritating and non-comedogenic.
It is available in a bottle of 15 ml along with a dropper.
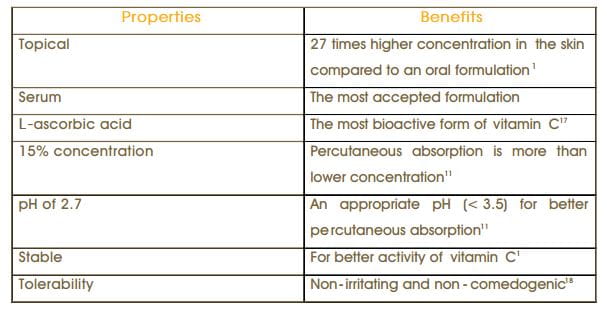
Table 2: VC 15 - an ideal formulation of Vitamin C
VC 15 is indicated for the following:
- Photodamaged/aging skin (prevention and cure)
- Dry skin
- Dull complexion, tough texture Fine
- lines and deep wrinkles
- Age spots
- Melasma/hyperpigmentation
- Acne and acne scars
- Post-procedure inflammation
VC 15 should be used once daily in the morning. The user should be instructed as
follows: Before application, ensure that the skin area to be treated and your hands are thoroughly
clean. Apply the serum before using any sunscreen and/or make-up. Use within one month after opening the
bottle.


Some people may experience a slight tingling or stinging sensation after application of the serum,
but this effect diminishes with continuous use.
Excess application of VC 15 will not provide quicker or better results. So. please use only the
recommended dosage.
VC 15 is contraindicated in patients having a history ot hypersensitivity to vitamin C or any of the
ingredients in the formulation.
VC 15 is meant for external use only. Avoid direct contact with the eyes or mucous membranes. Use
within 1 month after opening the bottle. Store between 15-30°C. Keep the dropper tightly screwed
on when not in use.
Due to the high concentration of L-ascorbic acid, there may be a temporary tingling or stinging
sensation after applying the product. If this occurs, avoid using the product on the most sensitive
facial areas including the sides of the nose and around the eyes.
Discontinue use of the product only if it has turned dark brown.
The only adverse effects reported are mild and typically resolve in the first 2 months
of therapy. These minor adverse effects included stinging (55%)
- erythema (24%). and dry skin (< 1%). 12
On the basis ol a solid foundation of in vivo, in vitro and animal model data, it can be stated that
vitamin C alleviates oxidative stress on the skin. Along with its antioxidant property it also has
photoprotective, depigmenting and anti-inflammatory properties. Vitamin C also provides the
additional advantages of replenishing vitamin E and stimulating dermal collagen synthesis, a major
target in chronic photoaging.
A significant body of scientific research supports the use and valuable role of topical vitamin C in
the treatment and prevention of photodamaged/aging skin. Topically applied vitamin C is also useful
for lightening hyper-pigmentation due to its depigmenting property. Due to its documented
anti-inflammatory properties, it is useful in treating inflammatory acne and post-procedure
inflammation. By promoting collagen synthesis, topical vitamin C improves fine lines and wrinkles.
In addition to these uses, topical vitamin C can be used as an adjunct to sunscreen for
photoprotection.
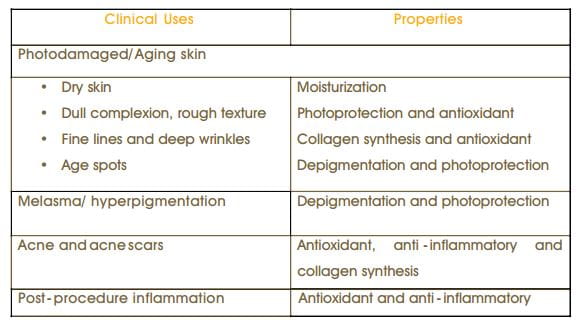
Table 3: Properties supporting clinical uses of topical vitamin C
Because of the diverse biologic effects of Ihis compound topical vitamin C has become a useful part of
the dermatologist's armamentarium.
1. Burke KE. Interaction of vitamins C and E os better cosmeceuticals.
Dermatologic Therapy 2007; 20:314-21.
2. Farris PK. Topical Vitamin C: A Useful Agent for Treating Photoaging and Other Derma tologic
Conditions. Dermatol Surg 2005; 31:814-18.
3. Colven RM.. Pinnell SR. Topical Vitamin C in aging. Clin Dermatol 1996; 14:227-34.
4. Phillips CL, Combs SB, Pinnell SR. Effects of ascorbic acid on proliferation and collagen
synthesis in relation to donor age of human dermal fibroblasts. J Invest Dermatol
1994;103:228-32.
5. Davidson JM, Luvalle PA, Zoia O, et al. Ascorbate differentially regulates elastin and collagen
biosynthesis in vascular smooth muscle cells and skin fibroblasts by pretranslational mechanisms. J
Biol Chem 1997; 272:345-52.
6. Humbert PG, Haftek M, Creidi P et al. Topical ascorbic acid in photoaged skin. Clinical
topographical and ultrastructural evaluation: Double-blind study vs. placebo. Exp Dermatol 2003;
12:237-44.
7. Darr D, Combs S, Dunsten S et al. Topical vitamin C protects porcine skin from ultra violet
radiation-induced damage. Br J Dermatol 1992; 127:247-53.
8. Carcamo JM, Pedraza A, Borquez-Ojeda O, Golde DS. Vitamin C suppresses TNF alpha-induced NF-kappa
B activation by inhibiting I kappa B alpha phosphorylation. Biochem 2002; 41:12995- 30002.
9. Alster T, West TB. Effect of vitamin C on postoperative C02 laser resurfacing erythema. Dermatol
Surg 1998; 24:331-34.
10. Espinal-Perez L, Moncada B, Castanedo-Cazares R A double-blind randomized trial of 5% ascorbic
acid vs 4% hydroquinone in melasma. Int J Dermatol 2004; 43:604-7.
11. Pinnell SR et al. Topical L-ascorbic acid: percutaneous absorption studies. Dermatol Surg 2001
Feb;27(2):137-42.
12. Traikovich SS. Use of topical ascorbic acid and its effects on photodamaged skin topography.
Arch Otolaryngol Head Neck Surg 1999;125:1091 -8.
13. Fitzpatrick Richard E. and Rostan Elizabeth F. Double-Blind, Half-Face Study Com paring Topical
Vitamin C and Vehicle for Rejuvenation of Photodamage. Dermatol Surg 2002:28:231-236.
14. Woolery-LIoyd H, Baumann L, Ikeno H. Sodium L-ascorbyl-2-phosphate 5% lotion for the treatment
of acne vulgaris: a randomized, double-blind, controlled trial. J Cosmet Dermatol. 2010
Mar;9(l):22-7.
15. Hiroshi Ikeno, Kitaro Ohmori, Shunji Yunoki. Takeshi Nishikawa. Open study comparing 5% sodium
L-ascorbyl-2-phosphate lotion versus 1 % clindamycin phosphate lotion for acne vulgaris. Cosmetic
Derm 2006; 19(1): 43-48.
16. Ruamrak C, Lourith N, Natakankitkul S. Comparison of clinical efficacies of sodium ascorbyl
phosphate, retinol and their combination in acne treatment. Int J Cosmet Sci.
2009Feb;31(l):41-6.
17. Lupo MR Antioxidants and vitamins in cosmetics. Clinics in Dermatology 2001; 19:467-473.
18. Data on file, Cipla Ltd.