

Hepatitis B virus (HBV) infection, which results in acute and chronic hepatitis B disease, is one of the most serious and prevalent health problems, affecting more than 2 billion people worldwide, with an estimated worldwide mortality of 0.5 to 1.2 million deaths a year. 1 The disease spectrum of HBV infection ranges from asymptomatic, mild infection to severe, progressive liver disease. 2,3 Chronicity is a serious issue with HBV infection since an estimated 15-25% of affected individuals die prematurely of liver cirrhosis or hepatocellular carcinoma. 4
Tenvir (Tenofovir disoproxil fumarate) - Product Monograph

6 Feb, 11


Unbeatable
Power in Treating Chronic Hepatitis B
Hepatitis B Virus Overview
Epidemiology
Although highly effective vaccines against HBV have been available since 1982, there are still more than 350 million chronic carriers. 5 Of these, 75% reside in the Asia Pacific region. 6 People with hepatitis B are at increased risk of developing hepatic decompensation, cirrhosis, and hepatocellular carcinoma. India contributes nearly 10% carriers to the world. Nearly 1 million HBV infections are added to the HBV pool in India yearly, contributing to its rapid expansion. 7
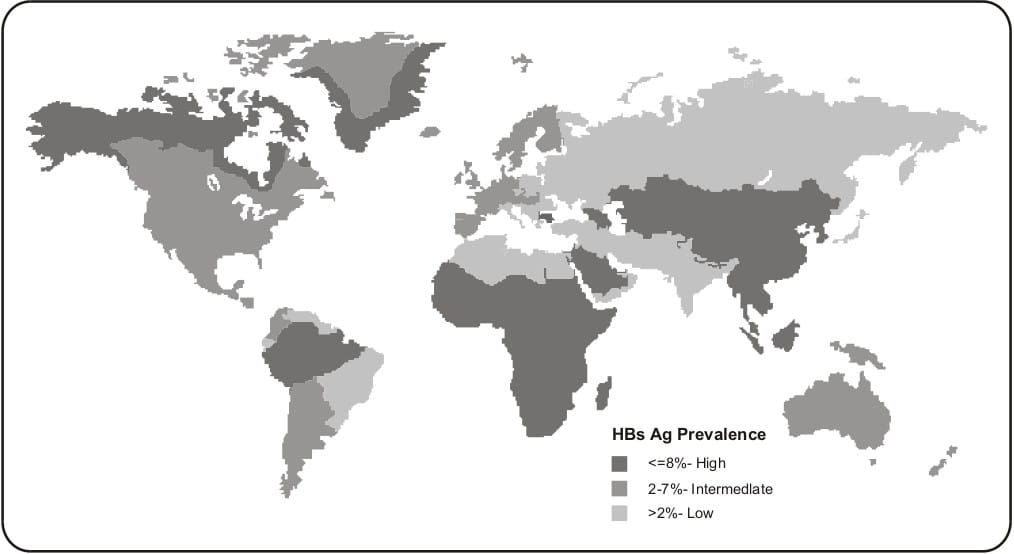
The global prevalence of chronic HBV infection varies widely, ranging from high levels (≥8%, e.g., Africa, Asia and the western Pacific) to intermediate (2-7%, eg, southern and eastern Europe) and low levels (<2%, eg, western Europe, North America and Australia) 8 (see Fig.1.1).
India lies in the intermediate zone of HBV prevalence. Transmission of HBV results from exposure to infectious blood or body fluids containing blood. Possible forms of transmission include (but are not limited to) unprotected sexual contact, blood transfusions, re-use of contaminated needles and syringes, and vertical transmission from mother to child during childbirth. 9, 10
Fig. 1.1: Global prevalence of chronic HBV infection
Hepatitis B Virus
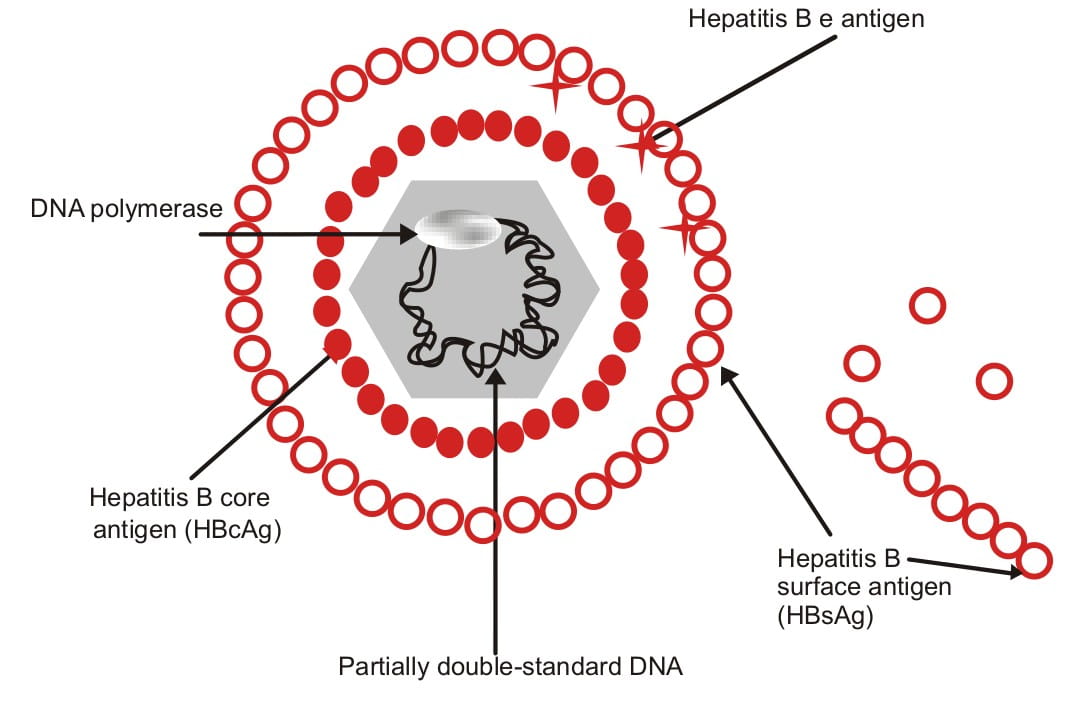
HBV is a DNA virus belonging to the class, Hepadnaviridae, and primarily infects the liver cells. In structure, the outer wall of the virus has envelope proteins known as hepatitis B surface antigens (HBsAg), as well as another antigen, the hepatitis B e antigen (HBeAg). The inner wall contains the hepatitis B core antigen (HBcAg). The nucleus has a partially double-stranded DNA with a DNA polymerase enzyme, both of which play an important role in the replication of the virus (see Fig. 1.2).
Fig. 1.2: Structure of HBV
HBV Genotypes
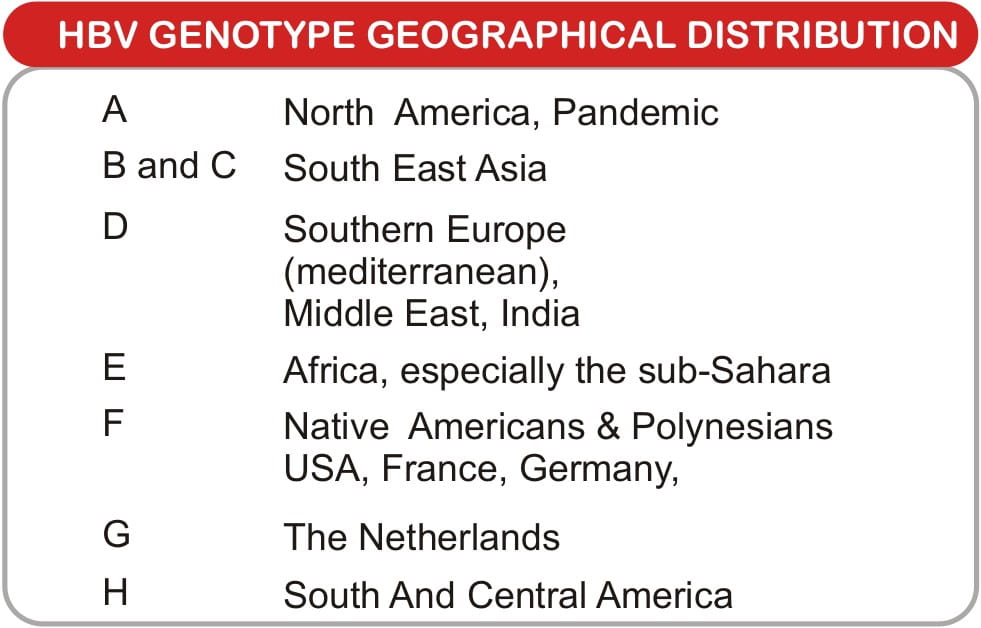
HBV has eight designated genotypes (A-H), based on the genome sequence divergence. Each genotype has its distinct geographic and ethnic distribution (see Table 1.1). Differences between the genotypes affect the disease severity, course and likelihood of complications, and the response to treatment. 11
Table 1.1: Geographical distribution of HBV genotypes 12
Influence of HBV genotypes on the response to antiviral therapy
The response to interferon therapy is better in individuals infected with genotypes A and B whereas no such particular difference has been noted in the response to oral antiviral drugs used in chronic HBV. 13
HBV Mutants
HBV has a mutation rate that is approximately 10 times higher than other DNA viruses and the reverse transcriptase lacks a proofreading function that is common to most other polymerases. This leads to the emergence of viral variants. Certain strains of these HBV variants may affect disease progression and therapeutic response. 14 The important ones among them are described below.
Pre-core and core mutant HBV
- These HBV variants appear during HBeAg seroconversion and they carry mutations in the pre- core region that prevent HBeAg synthesis, despite continuing production of infectious virions. This mutation is more prevalent in geographic regions areas where genotypes B, C, and D are predominant, such as Asia and the Mediterranean area region, where it can be detected in more than 50% of individuals with chronic hepatitis B. 15
- Core promoter variants express less HBeAg through transcriptional down regulation, which results in a substantial decrease in HBeAg expression, but enhanced viral genome replication.
- Prevalence of the core promoter variant is about 40%; it is evenly distributed among the major HBV genotypes.
- The type of disease without the HBeAg antigen is known as HBeAg-negative Chronic Hepatitis B. HBeAg-negative Chronic Hepatitis B has a more variable course than HBeAg-positive Chronic Hepatitis B, especially the core promoter mutations, which are associated with fluctuations in viremia, disease activity, recurrent relapses and higher, faster progression to cirrhosis. 16
HBV DNA polymerase variants
These may arise during HBV therapy with antiviral agents that target the viral DNA polymerase. 17 A well-known example would be the HBV variants with mutations within the tyrosine-methionine-aspartate-aspartate (YMDD) motif of the HBV DNA polymerase, which emerge as a result of selective pressure during lamivudine therapy. 18
Chronic Hepatitis B
An estimated 90% of adults with healthy immune systems will recover successfully from an acute HBV infection and develop positive surface antibodies that will protect them against future infections.
Chronic Hepatitis B Disease Progression and Complications
- Infection with HBV (HBsAg-positive) for more than 6 months is defined as chronic infection i.e., Chronic Hepatitis B.
- Approximately 5-10% of infected adults will develop chronic infections, which increases their risk for cirrhosis, liver failure or liver cancer (hepatocellular carcinoma)
- Infants have only a 10% chance of recovering from an acute infection and young children have up to a 50% chance of recovering, i.e., a much higher risk of progressing to a chronic infection when first infected with hepatitis. 19, 20
- Damage during chronic infection increases hepatocyte turnover, induces fibrosis and increases the chance of hepatocellular transformation and malignancy. 19
Markers of HBV Infection
The four markers of HBV infection are serological markers, virological loads (HBV DNA levels), biochemical markers of liver diseases and, finally, histological markers, i.e., liver biopsy (Fig.1.3).
Fig. 1.3: Markers of HBV infection
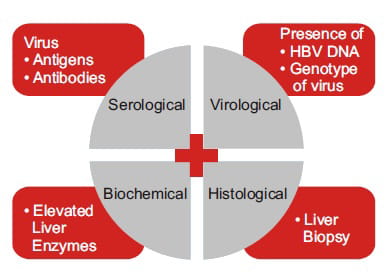
Table 1.2: Serological and virological markers of HBV infection 21
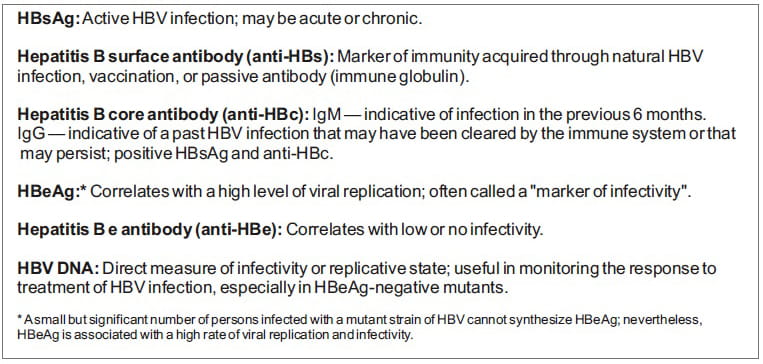
These antigens, as well as the corresponding antibodies produced by the immune system, serve as useful laboratory markers of past, current or chronic infections.
Biochemical evaluation of liver disease
Liver function is assessed with the following:
- Liver enzymes alanine transaminase (ALT) or sometimes aspartate transaminase (AST), serum albumin, serum prothrombin time and serum bilirubin.
Histological markers of liver disease
- A histological evaluation of Chronic Hepatitis B using liver biopsy is the most sensitive and accurate test done to aid the diagnosis of liver disease, assess the severity of known liver disease and monitor the progress of treatment. 22 However, it is not so commonly used given its invasive nature.
- Scores used to assess liver biopsy include the Histological Activity Index (HAI), or the Knodell Score used in clinical trials 25 and to assess changes in pathology following therapeutic intervention methods like the METAVIR system. 23, 24
Criteria for the initiation of Treatment in Chronic Hepatitis B 13, 26, 27
HBeAg-Positive Chronic Hepatitis B
In patients with HBeAg-positive Chronic Hepatitis B, treatment is clearly indicated when the serum HBV DNA is equal to 20,000 IU/mL (10 5 copies/mL) and the ALT level is persistently elevated (should be at least 2 x the upper limit of normal range [ULN] after 3-6 months of monitoring.
HBeAg-Negative Chronic Hepatitis BHBeAg-negative patients tend to have lower levels of serum HBV DNA than their HBeAg- positive counterparts, but may still have active disease. As a result, a lower HBV DNA threshold of 2000 IU/mL (10 4 copies/mL) coupled with a persistently elevated serum ALT after 3-6 months of monitoring (defined as >2 x ULN) should be considered for the initiation of treatment.
Treatment Endpoints
The ultimate goal of treatment is to suppress the HBV DNA to the lowest possible level, i.e., undetectable level, and prevent the progression of liver disease to liver failure, cirrhosis or hepatocellular carcinoma. For HBeAg-positive Chronic Hepatitis B, HBeAg seroconversion (loss of HBeAg and development of anti-HBe) with undetectable HBV DNA is generally regarded as the endpoint of therapy. For those with HBeAg-negative Chronic Hepatitis B, there is no serological endpoint; hence, the reduction of serum HBV DNA to undetectable levels may be an appropriate endpoint. 26,27,28
As per Asian-Pacific consensus statement on the management of chronic hepatitis B -2008, for oral antiviral agents, in HBeAg-positive patients treatment can be stopped when HBeAg seroconversion with undetectable HBV- DNA has been documented on 2 separate occasions at least 6 months apart. In HBeAg-negative patients, it is not clear how long this treatment should be continued, but treatment discontinuation can be considered if undetectable HBV-DNA has been documented on three separate occasions 6 months apart. 27
Current Treatments for Chronic Hepatitis B
There are now seven drugs approved by the U.S. Federal Drug Administration (FDA) for the treatment of Chronic Hepatitis B: Standard interferon alpha (IFN-alpha)-2b, pegylated IFN- alpha-2a, lamivudine, adefovir dipivoxil (adefovir), entecavir, telbivudine and tenofovir disoproxil fumarate (tenofovir DF).
Pegylated IFN-alpha-2a and standard IFN- alpha-2b
Pegylated IFN-alpha-2a has essentially replaced standard IFN-alpha-2b in clinical practice due to improved tolerability and efficacy with weekly dosing as compared to thrice-a-week dosing with standard IFN-alpha-2b. 29, 30 Pegylated IFN-alpha therapy is more effective in patients with low-level HBV DNA 20,000-10 million IU per mL, elevated ALT (especially if >90 IU/mL), immunocompetence, genotype A and B, normal liver function (albumin, bilirubin and coagulation), and acquisition of the infection in adulthood. It is indicated for 48 weeks in HBeAg-positive patients (27% HBeAg seroconversion at 48 weeks) and may be used in HBeAg-negative patients who have the best chance of a sustained response when off treatment. 31 Long-term use is problematic due to the side effects, the cost of treatment and the need for subcutaneous administration. Also, as interferons are immunomodulators, they cannot be used in patients with hepatic decompensation. 32
Oral antivirals
The increasing number of studies on oral antivirals has greatly expanded the options for HBV treatment. Till date, lamivudine and adefovir were being used as first-line agents, but with significant data on tenofovir DF and entecavir which are safe and achieve around 21% HBeAg loss at 2 years along with histological improvement in the majority of patients, things are expected to change. 33
There is significant efficacy and safety data on tenofovir DF from large randomized trials and the European Association for the Study of the Liver (EASL) Clinical Practice Guidelines, 2009, recommend tenofovir DF as a first-line drug in patients with chronic HBV. Tenofovir DF promises to be a potent option with a high barrier to resistance, and a highly efficacious, safe and well tolerated agent.
Clinical Pharmacology of Tenofovir
Tenofovir DF (tenofovir disoproxil fumarate) is the latest U.S. FDA-approved antiviral for the treatment of Chronic Hepatitis B. The clinical efficacy, safety and resistance profile of tenofovir DF offers important benefits over the existing oral antiviral agents.
Tenofovir DF Pharmacodynamics
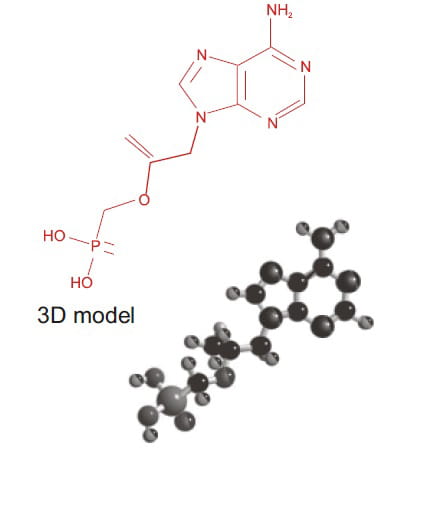
TENVIR is the brand name for tenofovir DF (a prodrug of tenofovir), which is a fumaric acid salt of bisisopropoxycarbonyloxymethyl ester derivative of tenofovir. Tenofovir DF exhibits activity against HIV-1 reverse transcriptase and HBV polymerase. It has the following structural formula (see Fig. 2.1).
Fig. 2.1: Chemical formula of tenofovir DF
Dosage Form
TENVIR Tablets are for oral administration. Each tablet contains 300 mg of tenofovir DF, and is to be taken once daily.
Mode of Action
Tenofovir DF is a potent inhibitor of HBV DNA polymerase. It requires an initial diester hydrolysis for conversion to tenofovir and subsequent phosphorylations by cellular enzymes to form tenofovir diphosphate (TFV- DP). TFV-DP is a weak inhibitor of mammalian DNA polymerases alpha, beta, and mitochondrial DNA polymerase gamma. 34
Spectrum of Antiviral Activity
In vitro activity
Tenofovir DF has selective activity against retroviruses and hepadnaviruses (duck HBV and human HBV) in vitro . 35 Tenofovir DF is efficiently phosphorylated to TFV-DP in both the HepG2 cells, which stably expressed the wild- type HBV and primary human hepatocytes. 36 TFV-DP has a long intracellular half-life (95 hours) and is a potent and competitive inhibitor of HBV polymerase (Ki = 0.18 μM). 37, 38, 39 In cell culture combination antiviral activity studies of tenofovir DF with the nucleoside anti-HBV reverse transcriptase inhibitors, emtricitabine,entecavir, lamivudine and telbivudine, no antagonistic activity was observed. 40
In vitro resistance profile
Tenofovir DF has demonstrated full activity against lamivudine-resistant HBV in vitro and clinically. Tenofovir DF retains activity against all of the major patterns of lamivudine- resistance mutations in vitro and clinically. 41 Tenofovir DF showed a small but reproducible decrease in susceptibility (3- to 4.2-fold) to clinical HBV isolates bearing rtN236T, the most common adefovir-associated resistance mutation. 42 The rtA194T HBV polymerase mutation recently identified in tenofovir DF- treated HIV/HBV-co-infected patients did not confer in vitro resistance to tenofovir DF as a single mutation or in a lamivudine-resistant viral background. The HepG2 cells were stably transfected with the wild-type or mutant HBV genomes with known telbivudine-resistance mutations, M204I and L80I/M204I. Telbivudine, lamivudine and entecavir lost 353- to >1000- fold activity whereas adefovir and tenofovir DF exhibited no more than 3- to 5-fold change. 43 On the basis of the data from cross-resistance and sensitivity testing in vitro and treatment outcomes, tenofovir DF proves to be a good treatment option for entecavir-resistant patients too. 44
In vivo activity
The antiviral effect of oral administration of tenofovir DF against chronic woodchuck hepatitis virus (WHV) infection, an established and predictive animal model for antiviral therapy, was evaluated in a placebo-controlled, dose-ranging study, which reduced serum WHV viremia significantly (0.2-1.5 log reduction from the pre-treatment level), intrahepatic WHV replication, and hepatic expression of WHV antigens. No evidence of toxicity was observed in any of the tenofovir DF- treated woodchucks. It was concluded that the oral administration of tenofovir DF for 4 weeks was safe and effective in the woodchuck model of chronic HBV infection. 45 Tenofovir DF has also been shown to inhibit the replication of duck HBV in primary duck hepatocytes with an IC 50 of 0.11 μM. 46
Tenofovir DF Pharmacokinetics 40
Pharmacokinetics in Healthy
Volunteers and HIV/HBV
Co-infected Individuals
Tenofovir DF pharmacokinetics is similar between these populations.
Absorption: The oral bioavailability of tenofovir DF in fasted patients is approximately 25%. The pharmacokinetics of tenofovir DF is dose-proportional over a dose range of 75 to 600 mg of tenofovir DF and is not affected by repeated dosing. Administration of tenofovir DF following a high-fat meal increases the oral bioavailability, with an increase of approximately 40% in the AUC and an increase of approximately 14% in the C max . Tenofovir DF can be taken orally without regard to food.
Distribution: In vitro binding of tenofovir DF to human plasma or serum proteins is less than 0.7% and 7.2%, respectively, over the concentration range of 0.01 to 25 μg/mL.
Metabolism and elimination: Tenofovir DF has no interaction with the cytochrome P450 (CYP450) 19, 20 system, and displays no hepatic metabolism. Tenofovir DF is eliminated by a combination of glomerular filtration and active tubular secretion, with 70-80% eliminated unchanged in the urine in 72 hours. There may be competition for elimination with other compounds that are also renally eliminated.
Pharmacokinetics in Special Populations
Tenofovir DF pharmacokinetics is similar in male and female patients. Pharmacokinetic studies have not been performed in children (<18 years of age) or in the elderly (>65 years of age).
Hepatic impairment
There were no substantial alterations in tenofovir DF pharmacokinetics in patients with hepatic impairment compared with unimpaired patients. No change in the dosage of TENVIR Tablets is required in patients with hepatic impairment.
Renal impairment
In patients with creatinine clearance <50 mL/min or with end-stage renal disease (ESRD) requiring dialysis, the C max and AUC of tenofovir DF were increased. It is recommended that the dosing interval for TENVIR Tablets be modified in patients with creatinine clearance <50 mL/min or in patients with ESRD who require dialysis.
Drug Interactions
No interaction with the CYP450 system and relevant drug interaction between tenofovir DF and other nucleoside/nucleotide analogs used for the treatment of HBV infections, such as lamivudine, adefovir, entecavir or emtricitabine, has been observed so far, but experience is lacking regarding the interaction between tenofovir DF and telbivudine and standard IFN- alpha-2b or pegylated IFN-alpha-2a. Co- administration with other drugs that are eliminated by tubular secretion, such as cidofovir, acyclovir, valacyclovir, ganciclovir, valaganciclovir and probenecid, may increase the serum concentrations of either tenofovir DF or the co-administered drug.
Summary: Clinical Pharmacology of Tenofovir
- Tenofovir DF is an oral prodrug of tenofovir.
- In vivo , tenofovir DF gets converted to its active form, tenofovir diphosphate, which intracellularly inhibits HBV polymerase.
- In vitro and in vivo , tenofovir DF shows activity against both the wild-type as well as the lamivudine-resistant variants of HBV .
- The pharmacokinetics of tenofovir DF are altered in patients with renal impairment, patients with creatinine clearance <50 mL/min or with ESRD requiring dialysis.
- Tenofovir DF does not inhibit CYP450 enzymes for Ki below 140 μM, thereby minimizing drug interactions.
- The oral bioavailability of tenofovir DF is approximately 25% in fasted patients and 40% after food uptake.
- The pharmacokinetics of tenofovir DF is independent over the dose range of 75 to 600 mg.
- Tenofovir DF is eliminated unchanged by a combination of glomerular filtration and active tubular secretion.
Clinical Efficacy of Tenofovir in Chronic Hepatitis B
Tenofovir DF has been successfully used in the treatment of HIV-infected patients and has demonstrated significant antiviral activity in both the wild-type and lamivudine-resistant HBV infections. It shows marked suppression of HBV replication below the detection limit in different patients groups with HBV mono- or HIV/HBV co-infection in most instances, with a remarkably high rate of HBeAg loss and even HBsAg loss. Several case reports describe the use of tenofovir DF as a rescue drug for patients with lamivudine resistance and severe reactivation of HBV infection. In all these instances, the use of tenofovir DF induced a rapid decline of viral DNA as well as ALT levels, followed by the recovery of liver function. Owing to its strong antiviral efficacy against both the wild-type and lamivudine/adefovir-resistant HBV infections, multidrug-resistant (HBV) mutations in treatment-na-ve and treatment- experienced patients, favorable resistance profile and low toxicity, tenofovir DF will certainly play an important role in the management of HBV infection.
HBV Monotherapy
Treatment-naïve Patients (Study 102 and Study 103)
Tenofovir DF treatment proves superior to adefovir in HBeAg-negative patients (Study 102) 47, 48 and HBeAg-positive patients with Chronic Hepatitis B (Study 103). 49, 50
Aim: To assess the 96-week efficacy and safety of tenofovir DF and of a switch to tenofovir DF after 48 weeks of adefovir in HBeAg-negative (N=375) and HBeAg-positive patients (N=266) with Chronic Hepatitis B mono-infection.
Study design: (Fig. 3.1)
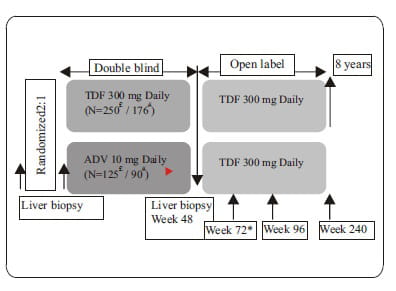
- Patients with HBeAg-negative or HBeAg- positive Chronic Hepatitis B mono-infection were randomized 2:1 to receive either tenofovir DF (TDF) 300 mg or adefovir (ADV) 10 mg once daily and it was a double blind study for the first 48 weeks.
- In Study 102, for the 48-week period, N=250 patients were on tenofovir DF and N=125 patients on adefovir.
- Similarly in Study 103, N=176 patients were on tenofovir DF (TDF) 300 mg and N =90 were on adefovir 10 mg once daily for the first 48 weeks.
- After 48 weeks, all patients (both tenofovir and adefovir groups) were switched to open- label tenofovir DF with a liver biopsy at week 48, for an additional 7 years in both study 102 and study 103.
- Option to initiate combination of emtricitabine plus tenofovir DF treatment at or after week 72 for confirmed HBV ≥ 69 IU/mL.
- Analyses were conducted at 48, 72 and 96 weeks.
- Liver biopsies were conducted at recruitment and at week 48.
Fig. 3.1: Study 102 and Study 103 of tenofovir DF in HBeAg-negative and HbeAg-positive
patients, respectively
Inclusion criteria:
- 18-69 years of age.
- Chronic Hepatitis B mono-infection.
- HBeAg-negative disease or HBeAg-positive disease.
- HBV DNA >10 6 copies/mL (HBeAg-positive) or HBV DNA >10 5 copies/mL
(HBeAg-negative) and ALT 2-10 x ULN (HBeAg-positive) or 1-10 x ULN
(HBeAg-negative) but no more than 10 times ULN in either. - Na-ve or lamivudine experienced.
- Knodell Necroinflammatory Score ≥3.
Subjects were treatment na-ve, defined as less than 12 weeks of treatment with any nucleoside or with the nucleotides tenofovir DF or adefovir dipivoxil, or treatment with lamivudine or emtricitabine of any duration. However, the protocol was amended to allow up to 120 subjects to enroll with more than 12 weeks of prior treatment with lamivudine or emtricitabine. Previous treatment with a nucleoside, nucleotide, or interferon (pegylated or not) must have ended 6 months prior to the required pretreatment liver biopsy. A total of 51 patients, 43 patients in study 102 and 8 patients in study 103 were lamivudine / emtricitabine experienced.
Exclusion criteria:
- Hepatitis delta virus (HDV), hepatitis C virus (HCV), HIV/HBV co-infection
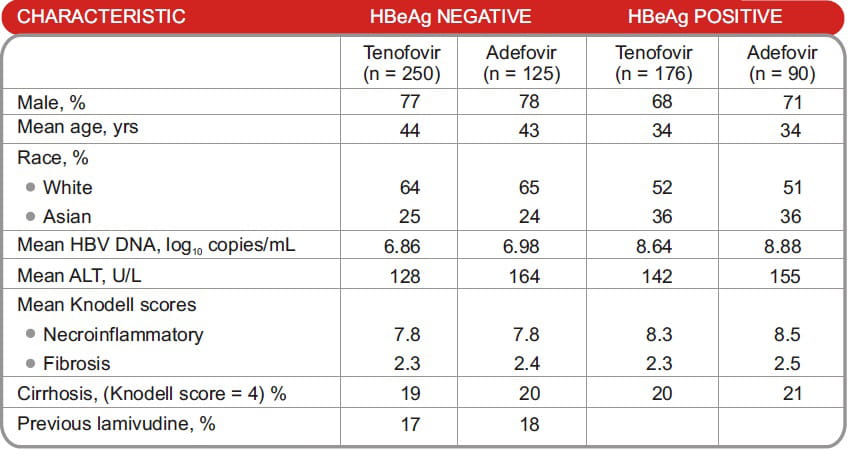
Baseline characteristics:
- Baseline demographics and disease characteristics were well balanced between the treatment arms (Table 3.1).
Table 3.1: Baseline characteristics in study 102 and study 103.
Results:
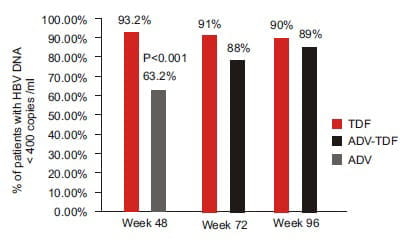
Study 102: Virologic response to tenofovir DF (Intent to treat [ITT])
- Virologic response was defined as HBV DNA <400 copies/mL or <69 IU/mL (Fig. 3.2). Three subjects (all in the TDF?TDF group) were switched to open-label emtricitabine/tenofovir during the open-label period due to confirmed viraemia. One of these 3 subjects had achieved complete viral suppression by Week 96.
- At the end of 96 weeks, both the continuous tenofovir DF group and the adefovir to tenofovir DF switch group showed undetectable HBV DNA levels in 90% and 89% of subjects, respectively.
Fig. 3.2: Virological response with HBV DNA Undetectability with tenofovir DF in Study 102 at
varied time intervals
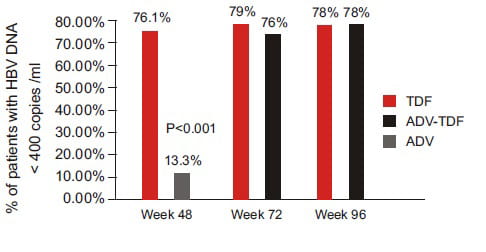
Study 103: Virological response (ITT) (Fig. 3.3)
- Sixteen subjects in the TDF?TDF group and 13 subjects in the ADV-TDF group switched to open-label emtricitabine/tenofovir during the open-label period due to confirmed viraemia.
Twenty-three of these subjects never achieved viral suppression < 400 copies/mL at any time during the study up to Week 96.
- At the end of 96 weeks, 78% of patients in both the continuous tenofovir DF group and the adefovir to tenofovir DF switch group showed undetectable HBV DNA levels.
Fig. 3.3: Virologic response and HBV DNA Undetectability with tenofovir DF in Study 103 at
varied time intervals.
Study 103: Serological response at week 96 (Fig. 3.4)
- At week 96, HBeAg loss was seen in 30% of patients in the continuous tenofovir DF group and 28% in the switch arm (adefovir to tenofovir DF).
- HBeAg seroconversion was seen in 26% of patients in the continuous tenofovir DF group and 24% in the switch arm (adefovir to tenofovir DF).
- HBsAg loss was 6% in both groups.
Fig. 3.4: Serological response at week 96 in Study 103
Study 102: Biochemical response
- Mean ALT values were similar at week 96 for adefovir-tenofovir DF and tenofovir DF- tenofovir DF patients, with an overall mean ALT value of 37 U/mL. Biochemical response at 48 and 72 weeks is shown in table 3.2.
Table 3.2: Biochemical response at 48 and 72 weeks in study 102
Study 103: Biochemical response
- At week 96, the overall mean ALT value was 36 U/L, with no significant differences between the groups. Biochemical response at 48 and 72 weeks is shown in table 3.3.
Table 3.3: Biochemical response at 48 and 72 weeks in study 103
Study 102: Histological response
- At week 48, both drugs produced similar histological responses in 72.4% of subjects in the tenofovir DF group and 68.8% in the adefovir group.
Study 103: Histological response
- At week 48, both drugs produced similar histological responses in 74.4% in the tenofovir DF group and 68% in the adefovir group.
Resistance profile: (Study 102 and Study 103)
- No tenofovir DF-resistance mutations were found through 96 weeks of tenofovir DF monotherapy.
Conclusion:
HBeAg-negative and HBeAg-positive patients
- In both groups, tenofovir DF produced potent, continuous viral suppression through 96 weeks.
- Tenofovir DF was well tolerated in HBeAg-positive and HBeAg-negative patients.
- Patients switching to tenofovir DF after 48 weeks of adefovir treatment had significant additional viral suppression similar to those treated with tenofovir DF for 96 weeks.
Nucleos(t)ide-resistant Patients
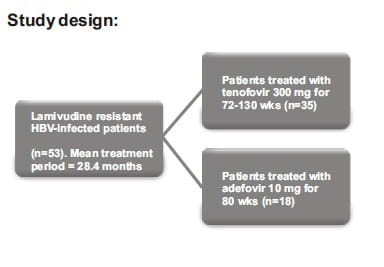
1. Lamivudine-resistant Patients
Tenofovir DF demonstrates significant antiviral activity in patients with lamivudine- resistant Chronic Hepatitis B. 51
Background: Patients with HBV infection require long-term treatment to clear the virus or prevent viral rebound. Despite the initial efficacy, extended treatment with lamivudine results in frequent lamivudine-resistant mutations. Adefovir, a nucleoside analog, has proven efficacy against wild-type and lamivudine-resistant HBV. Now, tenofovir DF is also approved for the treatment of Chronic Hepatitis B.
Aim: To compare adefovir and tenofovir DF for treating lamivudine-resistant Chronic Hepatitis B.
Study design:
Fig.3.5: Schematic representation of study
Inclusion criteria:
- Initial response to lamivudine ≥3 log decrease in HBV DNA.
- Normalized ALT.
- Genotypic and phenotypic evidence for lamivudine resistance.
- Treatment-na-ve for adefovir and tenofovir DF.
- Lack of HCV and HDV co-infection.
- No reported co-morbidities.
Laboratory evaluations:
- Serum HBV DNA was measured at baseline, weekly through week 4, and monthly for the duration of the HBV mutational analysis.
- Early viral kinetics was conducted on 5 adefovir and 5 tenofovir DF patients.
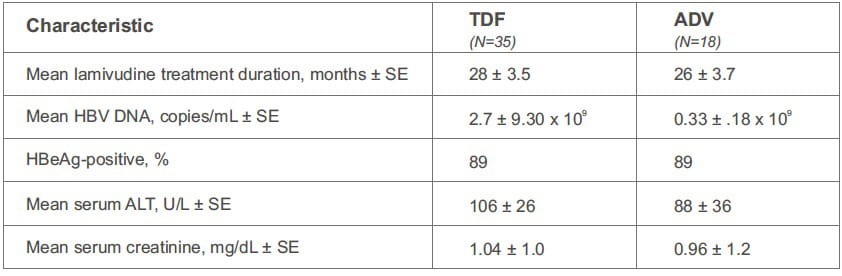
Baseline characteristics:
Baseline characteristics were similar among the groups (Table 3.4).
Table 3.4: Baseline characteristics in the study
Results:
Virological response to tenofovir DF (Table 3.5)
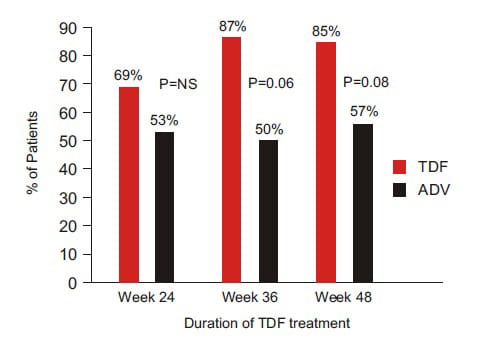
- Treatment with tenofovir DF led to a greater number of patients with <10 5 copies HBV DNA/mL or a higher limit of detection than adefovir (Fig. 3.6)
Viral kinetics: Trend toward more rapid HBV DNA level decline in patients receiving tenofovir DF (P = .085).
35-day decline for tenofovir DF, 2.9 log 10 copies/mL (N=5).
35-day decline for adefovir, 1.9 log 10 copies/mL (N=5).
Table 3.5: Virological response to tenofovir DF at various intervals
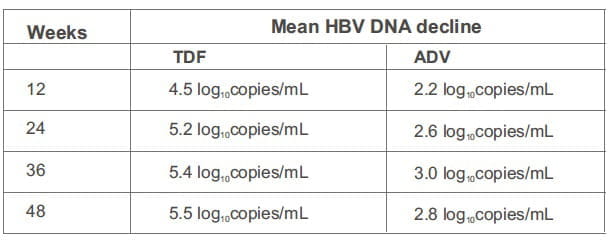
Fig. 3.6: Percentage of adefovir- and tenofovir DF-treated patients with HBV DNA decline to a
level of <10 5 copies/mL or <400 copies/mL at weeks 12, 24, 36, and 48, respectively
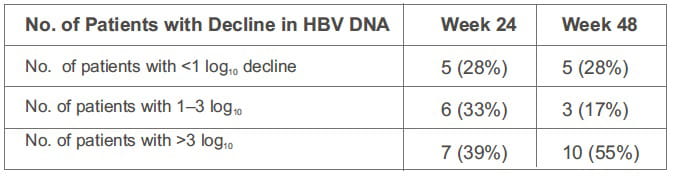
- Pronounced individual variations in HBV DNA levels observed with adefovir, but not tenofovir DF.
Table 3.6: HBV DNA decline in adefovir-treated patients
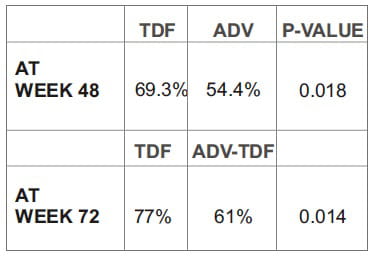
Biochemical response to tenofovir DF (Fig. 3.7)
- At the end of 48 weeks, ALT normalization was seen in 85% of the tenofovir DF group and in 57% of the adefovir arm.
Fig. 3.7: Biochemical response to tenofovir DF
Serological response to tenofovir DF
- HBeAg loss occurred in 35% of HbeAg -positive patients after a mean duration of 44 weeks (range: 24 to 76 weeks).
- HBsAg loss occurred in 14% of tenofovir DF- treated patients after a mean duration of 59 weeks.
- In the adefovir group, 19% of HBeAg-positive patients lost HBeAg at week 56 and 1 patient lost HBsAg at week 60.
Conclusion:
- Tenofovir DF appears more effective than adefovir in treating lamivudine-resistant HBV.
- HBV DNA levels dropped below the limit of detection for all tenofovir DF-treated patients.
'Tenofovir DF has stronger antiviral activity than adefovir and, therefore, could serve as a therapeutic tool for the induction of complete remission in patients with lamivudine-resistant HBV infection.'
2. Lamivudine-resistant and Adefovir non-responders 52
Tenofovir DF proves significant in patients with lamivudine-resistant HBV infection and high HBV DNA levels during adefovir therapy.
Background: The introduction of the nucleoside analog, lamivudine, and the nucleotide analog, adefovir, largely improved the outcome in Chronic Hepatitis B patients by also preventing hepatitis decompensation or the development of hepatocellular carcinoma.
Aim: To investigate whether the efficacy of viral suppression could be improved by replacing adefovir with tenofovir DF in lamivudine- resistant patients.
Study design: Fig. 3.8
Fig.3.8: Study design for tenofovir DF (TDF) in lamivudine (LAM)-resistant and adefovir (ADV)
non-responders

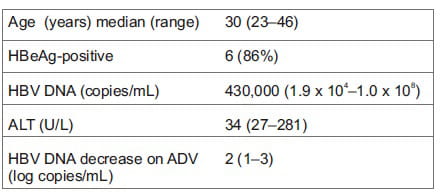
Baseline characteristics:
- HBV DNA levels at baseline adefovir ranged from 4.30 to 9.52 log 10 copies/mL.
- Mutations in the polymerase gene at baseline tenofovir DF were rtV173L, rtL180M, rtM204V and some others were infected with the wild-type virus.
- HBV DNA at baseline tenofovir DF ranged from 5.67 to 7.64 log10 copies/mL.
Results:
Virological response to tenofovir DF (Table 3.7)
Table 3.7: Virologic response to tenofovir DF at various time intervals

- Suppression of HBV DNA to an undetectable level (detection limit: 400 copies/mL) was achieved in 19 of the 20 patients after tenofovir DF treatment for a median duration of 3.5 months (range: 1 to 8 months).
Biochemical response to tenofovir DF:
- At the end of the observation period, 16 of the 20 patients had normal ALT values.
Serological response to tenofovir DF:
- HBeAg loss was seen in 4 patients.
- 1 patient seroconverted from HBsAg to anti- HBs at a titer of 1000 IU/mL in month 16.
Resistance profile of tenofovir DF:
- Mutations previously described as associated with adefovir resistance (rtA181V or rtN236T) were not present in any of the 20 patients.
- In addition, no other mutations were found in the polymerase gene.
- The presence of the mutations at rt180 and rt204 apparently had no influence on the efficacy of the consecutive tenofovir DF treatment.
Conclusion:
- These preliminary observations strongly suggest that tenofovir DF might be a highly effective rescue drug for HBV-infected patients with an altered responsiveness to treatment with lamivudine and adefovir.
'This follow-up study of patients with incomplete virological response to adefovir has demonstrated the superiority of tenofovir DF over adefovir in suppressing HBV replication in lamivudine-resistant HBV infection.'
3. Tenofovir DF in Entecavir-resistant Patients 44
Successful rescue therapy with tenofovir for an entecavir-resistant mutant in a Chronic Hepatitis B patient with pre-existent lamivudine resistance.
Background and aim: Entecavir has potent activity against HBV. Drug resistance has not been reported in nucleoside-na-ve patients and is low in lamivudine-refractory patients.
Case report:
A 43-year-old man was treated for HBeAg- positive Chronic Hepatitis B and liver cirrhosis (HBV DNA >
1-10 7 copies/mL at baseline ) with IFN alfa 5 MU thrice weekly for 30 weeks but he relapsed.
Interferon alfa was stopped and he was started on lamivudine 100mg/day. Initially HBV DNA became undetectable
and ALT normalized. After discontinuation of lamivudine HBV DNA levels rebounded accompanied by post treatment
flare. Reintroduction of lamivudine 100mg/day resulted again in a fast decline of HBV DNA to undetectable limit
and reduction in liver inflammation and HBeAg remained positive during treatment. After 230 weeks of continuous
lamivudine therapy, a hepatic flare was documented because of viral breakthrough.The viral load rebounded to
over 10 8 copies/mL. Twenty weeks later, entecavir 1mg daily was added to lamivudine regimen.
However, it took a year of combination therapy (69 weeks) to reduce viral levels to less than 103 copies/mL and
HBeAg loss occurred. After the viral load had been near the lower detection range of the polymerase chain
reaction (PCR), lamivudine was discontinued after 96 weeks of combination therapy. At week 144 of entecavir
treatment, after the HBV DNA had been below 10 3 copies/mL for over 70 weeks, a viral load of 5.69
-10 4 copies/mL was documented and HBeAg became positive again. Gradually the viral load increased to
1.27 -10 6 copies/mL.Treatment was switched from entecavir 1 mg daily, without overlap, to tenofovir
disoproxil 245 mg once daily.
After 25 days of treatment, a decline in the HBV DNA to below 1000 copies/mL was seen again and HBeAg seroconversion occurred after 6 weeks of therapy. The viral load continued to remain less than 10 3 copies/mL at the end more than 106 weeks.
Sequence analysis revealed the presence of rtL180M and rtM204V lamivudine resistance- associated mutations at the start of entecavir treatment. During entecavir treatment, the rtS202G mutation was selected.
Retrospective analysis revealed that during lamivudine treatment, three other mutations had been selected as well, namely, rtE1D, rtV207L, and rtI220L.
Conclusion:
- This case report describes the first case of entecavir resistance in a lamivudine-resistant patient with good initial suppression of viral replication for 70 weeks.
- Based on the data from cross-resistance and sensitivity testing in vitro and treatment outcomes, tenofovir DF proves to be a good treatment option for entecavir-resistant patients.
Compensated Cirrhosis
Tenofovir DF is Highly Active for the Treatment of Chronic Hepatitis B in Patients with Cirrhosis 53
Aim: To evaluate the efficacy and safety of tenofovir DF among patients with cirrhosis due to Chronic Hepatitis B participating in tenofovir DF pivotal Studies 102 (HBeAg-negative) and 103 (HBeAg-positive) and compare the consistency of response in cirrhotics versus non-cirrhotics at the end of 96 weeks.
Study design:
- Patients were randomized 2:1 to double-blind tenofovir DF 300 mg or adefovir 10 mg once daily for 48 weeks in Studies 102 (HBeAg- negative) and 103 (HBeAg-positive).
- Virologic (HBV DNA <400 c/mL [69 IU/mL]) and histological response (≥2-point decrease in the Knodell Necroinflammatory Score without worsening fibrosis) were prospectively evaluated.
- HBV DNA and safety laboratory parameters were performed every 4 weeks.
- For the subset analysis, the comparison of primary interest was tenofovir DF-treated cirrhotics versus non-cirrhotics through week 96.
Baseline characteristics:
- HBV DNA levels ranged from 6.81 to 7.87 log 10 c/mL IU/mL.
- The majority of the patients had a Knodell Necroinflammatory Score ≥5.
- ALT values ranged from 71-167 U/L.
- Nearly 40% of the patients were HBeAg- positive.
Results:
- HBV DNA <400 copies/mL was observed in 85% of patients, normalization of ALT at week 48 occurred in 69% of the patients and the histologicalresponse (measured by a 2-point drop in the Knodell Score) was observed in 79% of the patients on tenofovir DF (see Fig. 3.9).
- Greater virological response for tenofovir DF than adefovir was observed among cirrhotic patients at week 48.
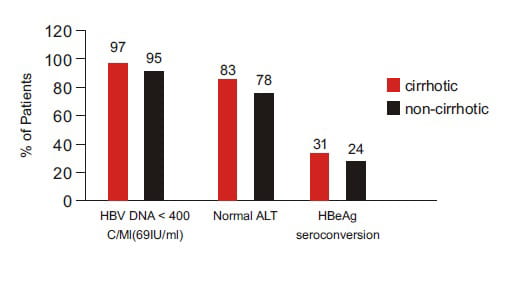
- Tenofovir DF produced a consistent response among cirrhotic and non-cirrhotic patients at week 96, with HBV DNA undetectable in 97% of cirrhotic patients (see Fig. 3.10).
Fig. 3.9: Virological, biochemical and histological response to tenofovir DF (TDF) in
cirrhotic patients at week 48 in comparison to adefovir (ADV)
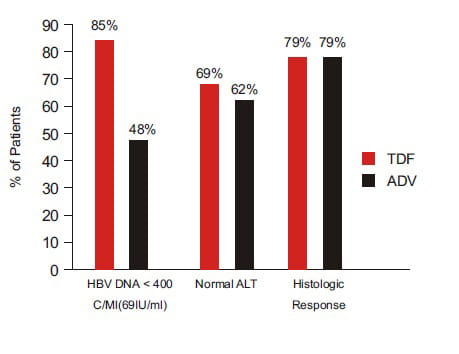
Fig. 3.10: Tenofovir DF produced a consistent response among cirrhotic and non-cirrhotic
patients at week 96
Conclusion:
- Tenofovir DF demonstrated high efficacy, good tolerability, and superior HBV DNA suppression compared with adefovir in subjects with compensated cirrhosis due to Chronic Hepatitis B.
'Tenofovir DF treatment in patients with cirrhosis was highly effective and led to similar levels of HBV DNA suppression, normalization of ALT and improvement of histological response in cirrhotic versus non-cirrhotic patients.'
Decompensated Cirrhosis
Successful Rescue Therapy with Tenofovir DF in a Patient with Hepatic Decompensation and Adefovir-resistant HBV Mutant 54
Background : In Chronic Hepatitis B, prolonged antiviral therapy with nucleoside analogs such as lamivudine is often necessary, but may result in the emergence of escape mutants which can be detected in as many as 70% of patients after 4 years of therapy.
Prolonged adefovir therapy exposes patients to the emergence of adefovir-resistant HBV mutants. Initial reports on the rtN236T mutation showed a preserved sensitivity to lamivudine; however, complex mutations are emerging with reduced susceptibility to lamivudine.
Case presentation:
In 1997, a 55-year-old Vietnamese man was diagnosed with HBV cirrhosis without HDV, HCV or HIV co-infections.
The route of infection probably was vertical transmission. Cirrhosis was confirmed by a liver biopsy and the
only complication was grade 1 esophageal varices (Child-Pugh score: A5).
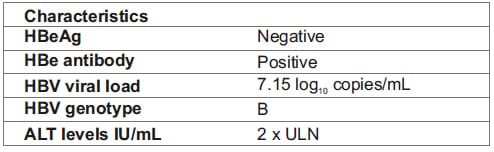
The patient's baseline characteristics were as in Table 3.8.
Table 3.8: Baseline characteristics of the study subject
The evolution of the HBV viral load is shown in Fig. 3.11 below:
Fig. 3.11: Evolution of HBV viral load
Case study:
- In 1997, a 55-year-old Vietnamese man was diagnosed with HBV cirrhosis without co- infections, with the only complication being grade1 esophageal varices (Child-Pugh score: A5). HBeAg was negative, anti-HBe positive, HBV viral load (HBV DNA) was 7.15 log 10 copies/mL and the HBV genotype B. ALT values were >2 ULN.
- In 1998, treatment with lamivudine 100 mg/day was started. After 3 months, HBV DNA was undetectable. Lamivudine was inadvertently stopped after only 10 months of treatment, and then started again in 2000 when a relapse occurred with a rise in HBV DNA to 5.75 log 10 and ALT values at 3.1 ULN. The next 2 years of treatment were uneventful, with undetectable HBV DNA and normal ALT values.
- In 2002, after 24 months of uninterrupted lamivudine treatment, HBV DNA became detectable by PCR (2.6 log 10 ), a viral breakthrough was documented (HBV DNA rose to 9.2 log 10 with ALT at 2.7 ULN).
- Sequencing of the HBV polymerase revealed two common lamivudine-resistant mutations - rtL180M and rtM204V. Adefovir 10 mg/day was added to the ongoing lamivudine. The evolution of the HBV viral load is as shown in Fig. 3.11. Over the next 10 months, HBV DNA never fell below 5 log 10 .
- In 2003, the HBV DNA titer was 5.28 log 10 . Lamivudine was then stopped, but adefovir was maintained; in addition, pegylated IFN-alfa-2a was introduced (180 ?g/week), but after five injections, the patient decided to stop pegylated IFN administration due to poor drug tolerance.
- Then, 15 months after stopping lamivudine, 13 months after stopping pegylated IFN treatment, and after 4 months of uninterrupted adefovir monotherapy, HBV DNA rose to 8.3 log 10 , ALT to 10 ULN and AST to 7 ULN. Two adefovir-resistant mutations, rtA181T and rtN236T, were detected, whereas the previous lamivudine- resistant mutations, rtL180M and rtM204V, were absent.
- A higher dose of adefovir (20 mg/day) was started. After 1 month, HBV DNA was at 7 log 10 and ALT levels remained unchanged. The patient's condition deteriorated with the occurrence of edema, ascites, jaundice, mild renal impairment (serum creatinine 110 μmol/L) and decreased prothrombin time (47% of normal).
- Tenofovir DF was then started at a dose of 300 mg/day, while adefovir was continued for 1 month at 10 mg/day and then stopped.
Results:
- After 2 months, HBV DNA became undetectable by PCR.
- Prothrombin time rose to 90% while jaundice and ascites resolved.
- After 8 months of tenofovir DF treatment, HBV DNA was still undetectable by PCR on three separate occasions.
- The patient is currently listed for a liver transplant.
Conclusion:
- Adefovir-resistant mutations can induce severe hepatic decompensation in cirrhotic patients and can be preceded by incomplete viral suppression.
- In these patients, close viral monitoring is mandatory. To avoid the emergence of resistant mutants, incomplete viral response to adefovir should prompt a change in antiviral treatment.
- Tenofovir DF is an effective treatment for adefovir-resistant mutants.
'The antiviral response to tenofovir DF was excellent. A rapid and sustained inhibition of viral replication, by sensitive PCR, was detected after only 2 months of treatment and resulted in an improvement in liver function.'
Post-Liver Transplant
Successful Tenofovir Therapy for Lamivudine Resistance Following Liver Transplant 55
Background: Resistant HBV strains develop in 30% of liver transplant recipients treated with lamivudine within 2 years from the time of the transplant. In nearly 70% of cases, it is common for liver transplant recipients to develop resistance within 3 years, often resulting in graft failure and/or patient death.
Aim: To assess the safety and outcomes of tenofovir DF salvage therapy for patients with lamivudine resistance in a retrospective cohort of liver transplant patients.
Study design: Fig.3.12
Fig.3.12 Schematic representation of study design
Methods: Medical records were retrospectively evaluated for patients who received tenofovir DF. Data collected included demographics, HBV serological information prior to and during tenofovir DF therapy, drug-related complications, and creatinine clearance. Criteria for lamivudine resistance included elevation of liver chemistries along with the reappearance of HBsAg, HBeAg, and/or HBV DNA.
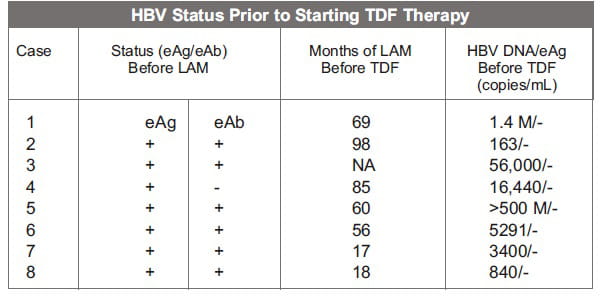
Table 3.9 summarizes the treatment data and biochemical results prior to liver transplant and with each viral breakthrough.
Table 3.9: Treatment information
Results:
Virologic and biochemical response to tenofovir DF after treatment
- Normalization of ALT levels occurred in the majority of patients.
- All 8 patients experienced HBV DNA viral suppression, with 7 having undetectable HBV DNA levels.
Conclusion:
- The results suggest that tenofovir DF safely and markedly decreases the replication of lamivudine-resistant HBV variants after liver transplant and is another potential option for the treatment of HBV lamivudine resistance.
'The results of this study show that tenofovir DF appears to be safe and effective for lowering HBV DNA in liver transplant patients suffering from HBV lamivudine resistance.'
Clinical Efficacy of Tenofovir in Chronic Hepatitis B
Combination Therapy
A concise rationale for multiple-drug therapy is that a resistance to monotherapy will occur eventually, with
serious consequences in some patients and grave public health implications over the long term. No data clearly
support de novo multiple-drug therapy.
The use of combination therapy is recommended in the following specific patient groups: Those with decompensated
cirrhosis, those co-infected with HIV/HBV and who are on antiretroviral therapy, those who have undergone liver
transplant, and those with treatment failure and drug-resistant HBV infection. 56
Tenofovir plus Emtricitabine
Significant Efficacy Seen Following a Switch to Tenofovir DF Combined with Emtricitabine in Patients with Chronic Hepatitis B Failing to Respond to Adefovir Monotherapy or an Adefovir-containing Regimen 57
Background: In patients with Chronic Hepatitis B, long-term use of lamivudine is limited by resistance mutations. Adefovir has a very low rate of resistance, but there have been recent reports describing resistance mutations. Tenofovir DF and emtricitabine show potent activity against wild-type and lamivudine- resistant HBV.
Aim: The aim of this study was to evaluate the efficacy of switching to combination therapy with tenofovir DF and emtricitabine in HIV- seronegative patients with Chronic Hepatitis B, who failed to achieve undetectable HBV DNA levels on adefovir.
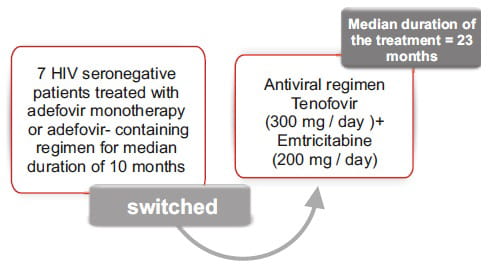
Study design: Fig.3.13
Fig.3.13 : Schematic representation of study design
Baseline characteristics:
Table 3.10: Baseline characteristics of the study group
Results:
Virological, biochemical and serological response to tenofovir DF
- This regimen change resulted in a median fall in HBV DNA levels of 3.0 log 10 copies/mL (range: 2 to 4) after a median treatment duration of 23 months (range: 14 to 28) (Table 3.11).
- All patients (100%) had achieved undetectable HBV DNA levels following combination therapy. Anti-HBe seroconversion occurred in 1 patient.
Table 3.11: Virologic, serological and biochemical treatment outcomes
Conclusion:
- In patients failing to respond to adefovir monotherapy or an adefovir-containing regimen for Chronic Hepatitis B, a combination of tenofovir DF and emtricitabine resulted in undetectable HBV DNA levels without any renal toxicity.
'Treatment with a combination of tenofovir DF and emtricitabine is well tolerated and results in virological and biochemical improvements without renal toxicity. This treatment regimen may be a useful therapeutic option in the setting of a suboptimal response or resistance to adefovir in HBV mono-infection.'
Summary: Clinical Efficacy of Tenofovir
- Tenofovir DF is a potent HBV inhibitor and has demonstrated efficacy in a wide spectrum of patient
populations, as follows:
- HBeAg-negative patients (Study 102)
- HBeAg-positive patients (Study 103)
- Wild-type and resistant HBV (resistant to drugs like lamivudine, adefovir and entecavir).
- Compensated and decompensated cirrhotic patients.
- Liver transplant patients.
- HIV/HBV co-infection.
- Tenofovir DF and emtricitabine combination in adefovir non-responders.
- High barrier to resistance, i.e. no resistance reported at the end of 2 years.
Clinical Safety and Tolerability of Tenofovir
Tenofovir DF has a well established, long-term safety profile in patients with HIV infection, with more than 2 million patient years of exposure. The safety data for the use of tenofovir DF in Chronic Hepatitis B-infected patients has been largely analyzed in Study 102 and Study 103 in treatment-na-ve HBeAg-negative and HBeAg- positive patients, respectively, and other subsets of the same study group, ie,lamivudine- experienced versus lamivudine-na-ve subjects and cirrhotics versus non-cirrhotics. In all the studies, tenofovir DF was generally well tolerated in patients with Chronic Hepatitis B. 48,50,53,55,58,59 In HBV-infected patients, the most common adverse reaction (all grades) was nausea (9%). 40
Tenofovir DF Safety in HBV Mono-infected Patients
In Phase III studies 102 and 103, HBeAg- negative or positive Chronic Hepatitis B patients were randomized 2:1 to double-blind, once-daily tenofovir DF 300 mg or adefovir 10 mg for 96 weeks. Following 96 weeks of tenofovir DF treatment, 7 (1.8%) of patients experienced some adverse event considered related to the study drug; however, no patient experienced a grade 3 or 4 adverse event and adverse events resulting in tenofovir DF discontinuation occurred in only 3 (<1%) patients. The reasons for discontinuation included malignant hepatic neoplasm, creatinine increase (peak: 1.3 mg/dL) and disturbance in attention, fatigue, and dizziness. Grade 3 and grade 4 laboratory abnormalities occurred in 8.7% of patients during open-label tenofovir DF and those occurring in >1% of patients included glucosuria, elevated serum amylase and elevated prothrombin time. During open-label tenofovir DF, no tenofovir DF patient treated for 96 weeks had a confirmed decrease in creatinine clearance to <50 mL/min, increase in creatinine of 0.5 mg/dL, or graded serum creatinine abnormality. No patient experienced bone fractures related to tenofovir DF. 48, 50, 58
In a subset of lamivudine-experienced patients in the same study (12 weeks of either lamivudine [N=49] or emtricitabine [N=2] experience; (Total N=51) was compared to lamivudine-na-ve patients (N=375). Serious adverse events considered related to tenofovir DF were 1.9% versus 3.9% in lamivudine-na-ve and lamivudine-experienced patients, respectively. Grade 3 or 4 adverse events considered related to tenofovir DF were 1.1% versus 2.0% in lamivudine-na-ve and lamivudine-experienced patients, respectively. Discontinuations due to adverse events were seen in 8 lamivudine-na-ve and 0 lamivudine experienced patients. Hypophosphatemia (confirmed phosphorus < 2mg/dL) was seen in 6 lamivudine-na-ve and 1 lamivudine- experienced patients. Confirmed 0.5 mg/dL increase in creatinine and confirmed creatinine clearance <50 mL/min was not seen in either of the groups. Tenofovir DF was well tolerated for up to 96 weeks in both lamivudine-experienced and lamivudine-na-ve patients. 48, 50, 59
Tenofovir DF demonstrated potent HBV DNA suppression and good tolerability in patients with compensated cirrhosis due to Chronic Hepatitis B through week 96. No patients experienced 0.5 mg/dL creatinine increase or creatinine clearance <50 mL/min. Hypophosphatemia was seen in 4% versus 1% in cirrhotic and non-cirrhotic patients, respectively. Hepatocellular carcinoma occurred in 1% of cirrhotic and 1% of non- cirrhotic patients. Grade 3 and 4 adverse events were seen in 11% versus 13% in cirrhotics and non-cirrhotics, respectively. No patient developed decompensated liver disease on tenofovir DF or adefovir. 48, 50, 53
Studies show that tenofovir DF appears to be safe and effective for lowering HBV DNA in liver transplant patients suffering from HBV lamivudine resistance. No adverse events were reported, and creatinine clearance was not impaired. Normalization of aminotransferase level tends to occur in the majority of the patients. 55
Treatment with tenofovir DF is associated with nephrotoxicity in some cases. Based on the results of clinical trials and postmarketing surveillance, a warning regarding renal impairment, including cases of acute renal failure and Fanconi syndrome, needs to be considered, especially in patients with pre- existing renal impairment. Besides this, tenofovir DF should be carefully used in patients with pre-existing risk factors for liver disease and a history of pathologic bone fracture, or those who are at risk for osteopenia, given its potential for causing severe hepatomegaly with steatosis and decrease in bone mineral density, respectively. These data demonstrate that tenofovir DF is extremely well- tolerated for various patient populations with Chronic Hepatitis B.
Summary: Safety Profile of Tenofovir .
- More than 12,000 patients have been treated with tenofovir DF alone or in combination with other antiretrovirals for periods ranging from 28 days to 215 weeks in Phase I-III clinical trials and expanded access studies.
- Tenofovir DF exhibits a low incidence of adverse effects, which have been shown to be often at the level of placebo.
- Tenofovir DF has shown no effect on the synthesis of mitochondrial DNA or the production of lactic acid in vitro .
- No significant alteration of kidney function was reported in clinical trials; however, occasional cases of kidney failure and Fanconi syndrome have been seen.
- A dosing interval adjustment is required for patients with creatinine clearance <50 mL/min.
- Tenofovir DF was well tolerated in Chronic Hepatitis B mono-infected patients.
- No major clinical side effects were reported during treatment with tenofovir DF in lamivudine- resistant patients.
- Tenofovir DF does not appear to be associated with nephrotoxicity in transplant patients with HBV when evaluated over a 12-month course.
- Tenofovir DF demonstrated potent tolerability in patients with compensated cirrhosis due to Chronic Hepatitis B.
Antiviral Resistance
Antiviral resistance is the major limitation of prolonged nucleos(t)ide analog therapy. Careful consideration is needed when selecting first-line therapy in order to avoid the emergence of resistance, especially the kind that may limit future treatment choices due to cross-resistance with other agents. 60 The risk factors for the emergence of drug-resistant mutants in the HBV DNA polymerase/reverse transcriptase increases with the following:
- Duration of therapy
- High baseline serum HBV DNA level
- Incomplete viral suppression during the first 6 months of therapy
- Non-compliance to therapy and prior exposure to nucleos(t)ide analogs
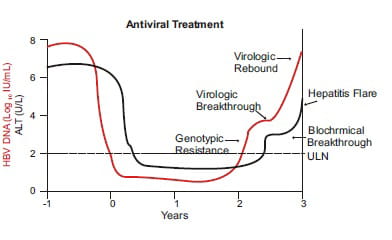
The first clinical manifestation of antiviral resistance is the virologic breakthrough, which is defined as >1 log 10 IU/mL increase in serum HBV DNA from the nadir in a patient who had an initial virologic response.
Serial changes in serum HBV DNA and ALT levels are seen in association with the emergence of antiviral-resistant HBV mutants. The first manifestation of antiviral resistance is the detection of resistant mutations (genotypic resistance). Resistant mutations may be detected at the same time or prior to a virologic breakthrough (increase in serum HBV DNA by ≥ 1 log 10 IU/mL from the nadir). With time, serum HBV DNA levels continue to increase (viral rebound) and ALT levels become abnormal (biochemical breakthrough). In some patients, the emergence of antiviral resistance leads to a marked increase in ALT (hepatitis flare) (see Fig. 5.1 below).
Fig.5.1: Manifestations of antiviral resistance
Lamivudine resistance 60, 61
- The widespread use of lamivudine has resulted in an increased prevalence of lamivudine-resistance mutations, detected in 10-15% of treatment-na-ve patients.
- Resistance to lamivudine emerges in higher rates in HIV/HBV co-infection, and more rapidly in patients with the HBV genotype A than the genotype D during the first year of infection.
- Lamivudine-resistance mutations confer broad cross-resistance to L-nucleosides, including telbivudine and several compounds in advanced clinical development (eg, emtricitabine, clevudine and valtorcitabine) and also confer cross-resistance to entecavir in vitro , requiring that a higher dose of entecavir (1 mg) be used clinically. Despite this higher dose and the potential requirement for acquiring a third resistance mutation, lamivudine-resistant patients frequently develop entecavir resistance, with more than half showing a genotypic resistance after 5 years of therapy. Given these data, entecavir is not currently considered an optimal treatment for lamivudine-resistant patients.
Adefovir resistance 60
- Viruses containing single or double adefovir- resistance mutations (rtA181V and/or rtN236T) demonstrate various levels of cross-resistance to tenofovir DF, lamivudine, telbivudine, and entecavir in vitro .
- Limited clinical data indicate that patients harboring adefovir-resistance mutations, particularly the rtN236T mutation, had a favorable antiviral response to lamivudine with a 2-6 log 10 decline in HBV DNA. Similarly, salvage therapy with entecavir in patients with adefovir-resistance mutations resulted in an initial 3-6 log 10 decline in HBV DNA. However, the majority of patients in these studies remained viremic following a switch from adefovir to either lamivudine or entecavir.
- In a recent study, 81% of patients failing adefovir therapy and who were treated with tenofovir DF achieved PCR-negative HBV DNA. Importantly, no significant differences in tenofovir DF responses were observed between patients with or without adefovir- resistance mutations at baseline. However, some studies have reported that patients harboring adefovir-resistance mutations may have a diminished response to tenofovir DF monotherapy, resulting in persistent levels of viremia.
Telbivudine resistance
- It has a similar barrier to resistance as lamivudine, but is more potent, which translates into a lower rate of resistance over a similar duration of therapy.
- Genotypic resistance to telbivudine after 1 year of therapy is 5% in HBeAg-positive patients and 2% in HBeAg-negative patients. 62
- Resistance to telbivudine is conferred by the rtM204I reverse transcriptase mutation, 63 but not the rtM204V. Serum HBV DNA level following 24 weeks of telbivudine treatment was a predictive marker for future development of resistant mutations after 2 years of treatment. 64
Entecavir resistance 60
- Failure of entecavir therapy due to resistance mutations (rtL180 M + rtM204V/I + T184, S202 or M250) is currently rare, but will probably increase with long-term use.
- At least one entecavir mutation (S202I) has also been observed in treatment-naïve patients. Not surprisingly, viral isolates with multiple lamivudine-resistance mutations plus the additional entecavir specific mutations show high level resistance to lamivudine and telbivudine in vitro . For this reason, neither lamivudine nor telbivudine therapy should be considered for patients who develop entecavir resistance. Adefovir and tenofovir DF retain in vitro efficacy against entecavir-resistant HBV.
- On the basis of its potency and recent approval, tenofovir DF may become the preferred therapy in this setting; however, the use of tenofovir DF to manage entecavir- resistant HBV needs to be explored further in the clinic.
Tenofovir DF resistance 61
- No firm data on HBV resistance-associated mutations selected during the course of tenofovir DF therapy exist.
- The rtA194T mutation in the B domain of the polymerase gene has been found to possibly be associated with resistance to tenofovir DF in 2 HBV/HIV-co-infected patients. However, an in vitro dose-response study found only a slight increase of tenofovir DF resistance (IC 50 ) caused by this mutation, thereby making a significant impact on its efficacy unlikely.
- The present lack of observation of HBV resistance against tenofovir DF is a strong argument in favor of the fact that, in the applied dosage, tenofovir DF generates a remarkably high genetic barrier against viral resistance.
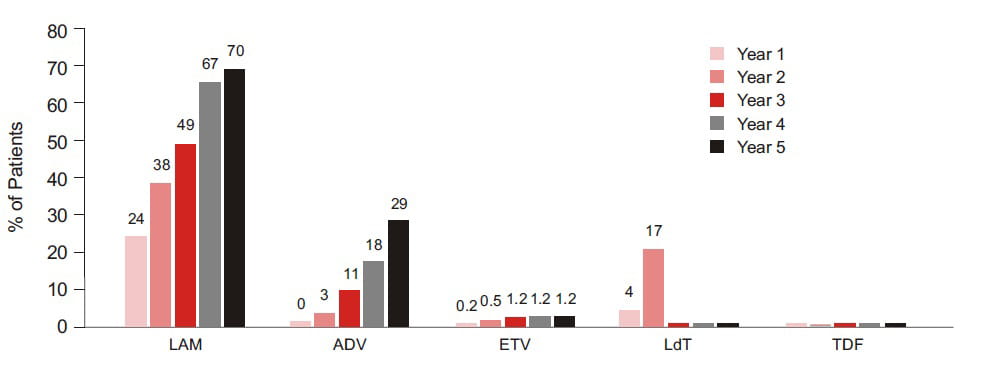
Fig.5.2: Cumulative Incidence of HBV resistance to lamivudine (LAM), adefovir (ADV), entecavir
(ETV), telbivudine (LdT) and tenofovir DF (TDF) in published pivotal trials in nucleos(t)ide-na-ve patients. These
trials included different populations, used different exclusion criteria and different follow-up endpoints.
65
Management of Antiviral-Resistant HBV-American Association for the Study of Liver Diseases (AASLD 2007)
Prevention
- Avoid unnecessary treatment.
- Initiate treatment with a potent antiviral that has a low rate of drug resistance, or with combination therapy.
- Switch to an alternative therapy in patients with primary non-response.
Monitoring
- Test for serum HBV DNA (PCR assay) every 3-6 months during treatment.
- Check for medication compliance in patients with virologic breakthrough.
- Confirm antiviral resistance with genotypic testing.
Place of Tenvir in Therapy
The latest EASL Clinical Practice Guidelines, 2009, clearly advocate the use of tenofovir DF confidently as first-line monotherapy and in other vital areas like drug resistance and primary non-response. Tenofovir DF finds a mention in some of the most trusted journals and articles.
'Characteristics of an ideal hepatitis B therapy include high potency and a very low rate of emerging viral
resistance. Only two of the currently approved nucleoside and nucleotide analogs, tenofovir and entecavir, have
these characteristics and, therefore, are superior to the other available oral agents.'
Current opinion in Gastroenterology 2009; 25:173-174.
'Tenofovir is not only a promising first-line treatment for nucleoside-naïve patients with chronic hepatitis B; it is also expected to be the key therapy (replacing adefovir and displacing entecavir) for lamivudine-refractory patients.' Anna S.F. Lok, Evolution of nucleoside/tide analogs for hepatitis B: Is the ideal drug here yet? doi:10.1016/j.jhep.2009.03.003
'In terms of antiviral activity against multidrug- resistance mutations, in vitro analysis indicates that tenofovir DF is far superior to the combination of lamivudine and adefovir, and has a marginal benefit over entecavir.' Hepatology 2005; 41:1391-1398.
'In terms of liver disease status, the rapid and strong antiviral efficacy of tenofovir makes it an
attractive rescue therapy for patients with liver cirrhosis.'
J Hepatol. 2005; 43 (6):937-943.
Tenofovir DF in Chronic Hepatitis B
( Ref: EASL Clinical Practice Guidelines, 2009 )
- Tenofovir DF and entecavir, with their high barrier to resistance, are potent HBV inhibitors; hence, both can be confidently used as first-line monotherapy.
- Lamivudine is an inexpensive agent, but has very high rates of resistance in monotherapy.
- Adefovir is more expensive than tenofovir DF, is less efficacious and has higher rates of resistance.
- Telbivudine, though a potent HBV inhibitor, has a low barrier to resistance, especially in patients with high baseline levels of replication and in those with detectable HBV DNA after 24 weeks of therapy.
Treatment Failure
- A rapid switch to tenofovir DF is recommended in primary non-response to oral antiviral drugs like adefovir.
- In partial virologic response at week 24 (for lamivudine, telbivudine, adefovir), switch to tenofovir DF, or add it to the existing drug, except with adefovir where such addition is not advised to avoid cross-resistance.
- In partial virologic response at week 48 to entecavir, add tenofovir DF.
Drug Resistance
Abbreviated Prescribing Information
PRODUCT NAME
TENVIR Tablets
ACTIVE INGREDIENT
Tenofovir disoproxil fumarate (tenofovir DF)
INDICATIONS
Treatment of Chronic Hepatitis B in adults with active viral replication, persistently raised liver enzymes (ALT
or AST), or histologically significant disease.
Efficacious in a wide spectrum of patients, namely, treatment-na-ve and nucleoside- resistant patients, patients with compensated or decompensated liver disease, patients awaiting liver transplant and HIV/HBV co- infected patients.
CONTRAINDICATIONS
Known hypersensitivity to tenofovir, tenofovir DF or any of their excipients.
WARNINGS AND PRECAUTIONS
Drug Interactions: Based on the results of in vitro experiments and the known elimination
pathway of tenofovir DF, the potential for CYP- mediated interactions involving tenofovir DF with other
medicinal products is low.
Hepatic Impairment: There were no substantial alterations in tenofovir DF pharmacokinetics in patients with hepatic impairment compared with unimpaired patients.
Renal Impairment: It is recommended that the dosing interval for tenofovir DF be modified in patients with creatinine clearance <50 mL/min or in patients with ESRD who require dialysis.
Pregnancy: Should be used only if the potential benefit clearly outweighs the potential risk to the fetus. Effective contraception should be used in women of childbearing age group when receiving tenofovir DF.
Lactation: Mothers should be instructed not to breastfeed if they are receiving tenofovir DF.
Undesirable Effects: Abdominal pain, diarrhea, headache, dizziness, fatigue, nasopharyngitis, back pain, and skin rash. Post-treatment elevations in ALT were seen in some patients.
DOSING AND ADMINISTRATION
In Adults (aged 18-65 years) for Chronic Hepatitis B: The dose of tenofovir DF is 300 mg once daily
taken orally, without regard to food.
Children (aged <18 years) or the Elderly (aged >65 years): Safety and efficacy not established sufficiently.
Renal Impairment: The dosing interval should be adjusted in patients with baseline creatinine clearance <50 mL/min.
Hemodialysis Patients: Every 7 days or after a total of approximately 12 hours of dialysis. Generally,
once weekly, assuming three hemodialysis sessions a week of approximately 4 hours duration.
TENVIR Tablets should be administered following the completion of dialysis.
OVERDOSAGE
In Study 901, 600 mg tenofovir DF was administered to 8 patients orally for 28 days. No severe adverse reactions
were reported. The effects of higher doses are not known.
If an overdose occurs, the patient must be monitored for evidence of toxicity and standard supportive treatment
applied as necessary.
Tenofovir DF is efficiently removed by hemodialysis, with an extraction coefficient of approximately 54%. Following a single 300 mg dose of tenofovir DF, a 4-hour hemodialysis session removed approximately 10% of the administered dose.
Full prescribing information available on request.
Unbeatable Power Proven by Two Landmark Trials - 102 & 103
- Studies 102 and 103 included a total of 641 Chronic Hepatitis B patients
- Both studies are scheduled to continue up to 8 years
- Both studies were presented at AASLD 2008 and week 48 data has been published in NEJM
- Results at 96-week clearly demonstrated tenofovir's superiority over adefovir dipivoxil
- US FDA approved tenofovir for chronic HBV based on results from these studies
References
1. Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and
emerging prevention and control measures. J Viral Hepatol 2004; 11: 97-107.
2. Sherlock S., Dooley J. Diseases of the liver and biliary system. 10th ed. Oxford: Blackwell Science, 1997.
3. Schiff E., Sorell M., and Maddrey W. Diseases of the liver. 8th ed Hagerstown: Lippincott Williams &Wilkins, 1999.
4. Mast E., Alter M. Epidemiology of viral hepatitis: An overview. Sem Virol 1993; 4:273-283.
5. Yun-Fan Liaw, Chia-Ming Chu. Hepatitis B virus infection. Lancet 2009; 373:582-92.
6. Merican I., Guan R., Amarapuka D., Alexander M.J., et al. Chronic hepatitis B virus infection in Asian countries. J Gastroenterol Hepatol. 2000 Dec; 15 (12):1356-61.
7. Chowdhury A. Epidemiology of hepatitis B virus infection in India. Hep B Annual 2004; 1:17-24.
8. Maddrey W.C. Hepatitis B: An important public health issue. J Med Virol. 2000 Jul; 61(3):362-6.
9. Petersen N.J., Barrett D.H., Bond W.W., Berquist K.R., Favero M.S., Bender T.R., Maynard J.E. (1976). "Hepatitis B surface antigen in saliva, impetiginous lesions, and the environment in two remote Alaskan villages". Appl. Environ.Microbiol. 32 (4): 572-574.
10. http://www.health.vic.gov.au/ideas/diseases/hepb. accessed in June 2009.
11. Liu C., Kao J. Hepatitis B virus genotypes: Epidemiology and therapeutic implications. Hep B Annual 2006; 3:54-75
12. Daryl T.-Y. Lau and Wissam Bleibel. Current status of antiviral therapy for hepatitis B. Therapeutic Advances in Gastroenterology.2008; 1(1) 61-75.
13. Keeffe E.B., Dieterich D.T., Han S.H., et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: An update. Clin Gastroenterol Hepatol 2006; 4:936-962.
14. Carman W. Molecular variants of the hepatitis B virus. Clin Lab Med 1996; 16:407-428.
15. Wai C.T., Fontana R.J. Clinical significance of hepatitis B virus genotypes, variants, and mutants. Clin Liver Dis. 2004; 8:321-352.
16. Tong S., Kyun-Hwan K., Chante C., Wands J., Li J. Hepatitis B virus e antigen variants. Int J Med Sci., 2005; 2:2-7.
17. Zoulim F. Therapy of chronic hepatitis B virus infection: Inhibition of the viral polymerase and other antiviral strategies. Antiviral Res 1999; 44:1-30.
18. Allen M.I. Identification and characterization of mutations in hepatitis B virus resistant to lamivudine. Hepatology 1998; 27 (6):1670-7.
19. Hollinger F.B., Liang T.J. Hepatitis B virus. In: Knipe D.M., Howley P.M., editors. Field's Virology. Fourth ed. Philadelphia, PA: Lippincott, Williams and Wilkins; 2001. pp. 2971-3036.
20. Robinson W.S. Hepatitis B virus and Hepatitis D virus. In: Mandell G.L., Nemmett J.E., Dolin R., editor. Principles and Practice of Infectious Diseases. New York: Churchill Livingstone; 1995. pp. 1406-1439.
21. http://www.gastroresource.com/GITextbook/en/Chapter14/14-4.htm. accessed May, 2009.
22. Grant A., Neuberger J. (October 1999). "Guidelines on the use of liver biopsy in clinical practice. British Society of Gastroenterology". Gut 45 Suppl 4: IV1-IV11.
23. The French METAVIR Cooperative Study Group. Intraobserver and interobserver variations in liver biopsy interpretation in patients with chronic hepatitis C. Hepatology 1994; 20:15-20
24. Bedossa P., Poynard T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology 1996; 24:289-293
25. Knodell R.G., Ishak K.G., Black W.C., et al. Formulation and application of a numerical scoring system for assessing histological activity in asymptomatic chronic active hepatitis. Hepatology 1981; 1:431-435
26. Lok A.S., McMahon B.J. AASLD Practice Guidelines: Chronic Hepatitis B. Hepatology., 2007; 45:507-539.
27. Liaw Y.F., Leung N., Kao J.H., et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2008 update. Hepatol Int., 2008; 2:263-283.
28. Malik A.H., Lee W.M. Chronic hepatitis B virus infection: Treatment strategies for the next millennium. Ann Intern Med 2000; 132:723-31.
29. Lok A.S., McMahon B.J. Chronic hepatitis B. Hepatology 2007; 45:507-539.
30. Cooksley W.G. Treatment with interferons (including pegylated interferons) in patients with hepatitis B. Semin Liver Dis 2004; 24:45-53.
31. Perrillo R.P. Therapy of hepatitis B - viral suppression or eradication? Hepatology 2006; 43 (suppl 1):S182-S193.
32. Hoofnagle Jay H. and Di Bisceglie Adrian M. The Treatment of Chronic Viral Hepatitis. 1997; 336:347-356.
33. http://www.hcvadvocate.org/hcsp/hcsp_pdf/HBV%20Treatment%20Overview.pdf as accessed in July 2009.
34. www.gilead.com/pdf/viread_pi.pdf as accessed in July 2009.
35. B-mmel Florian van and Berg Thomas. Role of tenofovir in the treatment of chronic HBV infection. Future Virol. 2008; 3 (3):207-220.
36. Ray A.S., Myrick F., Vela J. E., Olson L.Y., Eisenberg E. J., Borroto-Esodo K., Miller M. D., and Fridland A., 2005. Lack of a metabolic and antiviral drug interaction between tenofovir, abacavir and lamivudine. Antivir. Ther. 10:451-457.
37. Delaney William E., IV,* Ray Adrian S., et al. Intracellular Metabolism and In Vitro Activity of Tenofovir against Hepatitis B Virus Antimicrob. Agents Chemother. 2006; 7: 2471-2477
38. Xiong X., Yang H., Westland C.E., Zou R., and Gibbs C.S., 2000. In vitro evaluation of hepatitis B virus polymerase mutations associated with famciclovir resistance. Hepatology 31:219-224.
39. Xiong X., Flores C., Yang H., Toole J.J., and Gibbs C.S., 1998. Mutations in hepatitis B DNA polymerase associated with resistance to lamivudine do not confer resistance to adefovir in vitro. Hepatology 28:1669-1673.
40. http://www.accessdata.fda.gov/drugsatfda_docs/label/2008/021356s026lbl.pdf as accessed in July 2009.
41. Yang H., Qi X., Sabogal A., Miller M. D., Xiong S., and Delaney W. E., IV. 2005. Cross-resistance testing of next- generation nucleoside and nucleotide analogs against lamivudine-resistant HBV. Antivir. Ther. 10:625-633.
42. Brunelle M. N., Jacquard A. C., Pichoud C., Durantel D., Carrouee-Durantel S., Villeneuve J. P., Trepo C., and Zoulim F. , 2005. Susceptibility to antivirals of a human HBV strain with mutations conferring resistance to both lamivudine and adefovir. Hepatology 41:1391-1398.
43. Telbivudine, a nucleoside analog inhibitor of HBV polymerase, has a different in vitro cross-resistance profile than the nucleotide analog inhibitors, adefovir and tenofovir. Antiviral research. 2009; 81:147-155.
44. Selection of an entecavir-resistant mutant despite prolonged hepatitis B virus DNA suppression, in a chronic hepatitis B patient with pre-existent lamivudine resistance: Successful rescue therapy with tenofovir. European Journal of Gastroenterology & Hepatology 20 (8):773-777, August 2008.
45. Menne Stephan, Cote Paul J., Korba Brent E., et al. Antiviral Effect of Oral Administration of Tenofovir Disoproxil Fumarate in Woodchucks with Chronic Woodchuck Hepatitis Virus Infection . Antimicrobial Agents and Chemotherapy, 2005; 49:2720-2728.
46. Heijtink R.A., Kruining J., de Wilde G.A., Balzarini J., De Clercq E., Schalm S.W. Inhibitory effects of acyclic nucleoside phosphonates on human hepatitis B virus and duck hepatitis B virus infections in tissue culture. Antimicrob Agents Chemother 1994 Sep; 38 (9):2180-2.
47. Treatment with Tenofovir for 96 Weeks Results in High Rate of HBV DNA Suppression in Patients with HBeAg- NegativeChroniChronic Hepatitis BVInfection. http://www.clinicaloptions.com/Hepatitis/Conference%20Coverage/AASLD% 20 2008/Tracks/Approved%20HBV%20Agents/Capsules/146.aspx. accessed in June 2009.
48. Marcellin P., Buti M., Krastev Z., et al. Two-year tenofovir disoproxil fumarate (TDF) treatment and adefovir dipivoxil (ADV) switch data in HBeAg-negative patients with chronic hepatitis B (study 102), preliminary analysis. Program and abstracts of the 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31-November 4, 2008; San Francisco, California. Abstract 146.
49. Tenofovir Provides Effective and Sustained Virologic Suppression in HBeAg-Positive HBV-Infected Patients Through 96 Weeks.http://www.clinicaloptions.com/Hepatitis/Conference%20Coverage/AASLD%202008/Tracks/Approved%20HBV%20Agents/Capsules/158.aspx. accessed in June 2009.
50. Heathcote E., Gane E.J., de Man R.A., et al. Two-year tenofovir disoproxil fumarate (TDF) treatment and adefovir dipivoxil (ADV) switch data in HBeAg-positive patients with chronic hepatitis B (Study 103), preliminary analysis. Program and abstracts of the 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31-November 4, 2008; San Francisco, California. Abstract 158.
51. Van Bommel F., Wunsche T., Mauss S., et al. Comparison of Adefovir and Tenofovir in the treatment of lamivudine-resistant hepatitis B virus infection. Hepatology.2004; 40:1421-1425.
52. Tenofovir for Patients with Lamivudine-Resistant Hepatitis B Virus (HBV) Infection and High HBV DNA Level during Adefovir Therapy. Hepatology 2006; 44: 318-325.
53. Buti M., Hadziyannis S., Mathurin P., et al. i. Tenofovir disoproxil fumarate (TDF) is highly active for treatment of chronic hepatitis B in subjects with cirrhosis. 43rd annual meeting of the European Association for the Study of the Liver (EASL 2008). Milan, Italy. April 23-27, 2008. ii.Two-years safety and efficacy of tenofovir disoproxil fumarate (TDF) in patients with HBV-induced cirrhosis. Program and abstracts of the 44th Annual Meeting of the European Association for the Study of the Liver; April 22-26, 2009; Copenhagen, Denmark. Abstract 21
. 54. Case Report Successful Rescue Therapy with Tenofovir in a Patient with Hepatic Decompensation and Adefovir-Resistant HBV Mutant. Comparative Hepatology 2006, 5:1.
55. Neff G.W., Nery J., Lau D.T.Y., et al. Tenofovir Therapy for Lamivudine Resistance Following Liver Transplantation. Ann Pharmacother 2004; 38:1999-2004.
56. Terrault Norah A. Benefits and Risks of Combination Therapy for Hepatitis B. HEPATOLOGY 2009; 49:S122-S128.
57. Effect of switching to tenofovir with emtricitabine in patients with chronic hepatitis B failing to respond to an adefovir-containing regimen. Eur J Gastroenterol Hepatol. 18:1247-1253.
58. Marcellin P, Heathcote E J, Jacobson I, et al. Safety and Tolerability of 96 Weeks of Tenofovir Disoproxil Fumarate (TDF) Treatment in HBeAg-Negative and -Positive Patients Infected with Chronic Hepatitis B (Chronic Hepatitis B); 44th Annual Meeting of the European Association for the Study of the Liver; April 22-26, 2009; Copenhagen, Denmark.
59. Manns M., Jeffers L., Dalekos G., et al. The Antiviral Response To Tenofovir Disoproxil Fumarate (TDF) is Comparable in Lamivudine (LAM)-Na-ve and LAM-Experienced Subjects Treated for Chronic Hepatitis B (Chronic Hepatitis B) presented at EASL 2008 (#1587).
60. Review: Current status of antiviral therapy for hepatitis B. Therapeutic Advances in Gastroenterology 2008; 1; 61
61. Dusheiko B. G., Antonakopoulos N. Current treatment of hepatitis. Gut 2008; 57:105-124.
62. Lai C.L., Gane E., Liaw Y.F., et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007;357:2576-88.
63. Seifer M., Patty A., Serra I., Li B., Standring D.N. Telbivudine, a nucleoside analog inhibitor of HBV polymerase, has a different in vitro cross-resistance profile than the nucleotide analog inhibitors, adefovir and tenofovir. Antiviral Res., 2009; 81:147-155.
64. Liaw Y.F., Gane E., Leung N., et al. 2-Year GLOBE trial results: Telbivudine is superior to lamivudine in patients with chronic hepatitis B. Gastroenterology 2009; 136:486-495.
65. European Association for the Study of the Liver. Journal of Hepatology.2009; 50 227-242.
2. Sherlock S., Dooley J. Diseases of the liver and biliary system. 10th ed. Oxford: Blackwell Science, 1997.
3. Schiff E., Sorell M., and Maddrey W. Diseases of the liver. 8th ed Hagerstown: Lippincott Williams &Wilkins, 1999.
4. Mast E., Alter M. Epidemiology of viral hepatitis: An overview. Sem Virol 1993; 4:273-283.
5. Yun-Fan Liaw, Chia-Ming Chu. Hepatitis B virus infection. Lancet 2009; 373:582-92.
6. Merican I., Guan R., Amarapuka D., Alexander M.J., et al. Chronic hepatitis B virus infection in Asian countries. J Gastroenterol Hepatol. 2000 Dec; 15 (12):1356-61.
7. Chowdhury A. Epidemiology of hepatitis B virus infection in India. Hep B Annual 2004; 1:17-24.
8. Maddrey W.C. Hepatitis B: An important public health issue. J Med Virol. 2000 Jul; 61(3):362-6.
9. Petersen N.J., Barrett D.H., Bond W.W., Berquist K.R., Favero M.S., Bender T.R., Maynard J.E. (1976). "Hepatitis B surface antigen in saliva, impetiginous lesions, and the environment in two remote Alaskan villages". Appl. Environ.Microbiol. 32 (4): 572-574.
10. http://www.health.vic.gov.au/ideas/diseases/hepb. accessed in June 2009.
11. Liu C., Kao J. Hepatitis B virus genotypes: Epidemiology and therapeutic implications. Hep B Annual 2006; 3:54-75
12. Daryl T.-Y. Lau and Wissam Bleibel. Current status of antiviral therapy for hepatitis B. Therapeutic Advances in Gastroenterology.2008; 1(1) 61-75.
13. Keeffe E.B., Dieterich D.T., Han S.H., et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: An update. Clin Gastroenterol Hepatol 2006; 4:936-962.
14. Carman W. Molecular variants of the hepatitis B virus. Clin Lab Med 1996; 16:407-428.
15. Wai C.T., Fontana R.J. Clinical significance of hepatitis B virus genotypes, variants, and mutants. Clin Liver Dis. 2004; 8:321-352.
16. Tong S., Kyun-Hwan K., Chante C., Wands J., Li J. Hepatitis B virus e antigen variants. Int J Med Sci., 2005; 2:2-7.
17. Zoulim F. Therapy of chronic hepatitis B virus infection: Inhibition of the viral polymerase and other antiviral strategies. Antiviral Res 1999; 44:1-30.
18. Allen M.I. Identification and characterization of mutations in hepatitis B virus resistant to lamivudine. Hepatology 1998; 27 (6):1670-7.
19. Hollinger F.B., Liang T.J. Hepatitis B virus. In: Knipe D.M., Howley P.M., editors. Field's Virology. Fourth ed. Philadelphia, PA: Lippincott, Williams and Wilkins; 2001. pp. 2971-3036.
20. Robinson W.S. Hepatitis B virus and Hepatitis D virus. In: Mandell G.L., Nemmett J.E., Dolin R., editor. Principles and Practice of Infectious Diseases. New York: Churchill Livingstone; 1995. pp. 1406-1439.
21. http://www.gastroresource.com/GITextbook/en/Chapter14/14-4.htm. accessed May, 2009.
22. Grant A., Neuberger J. (October 1999). "Guidelines on the use of liver biopsy in clinical practice. British Society of Gastroenterology". Gut 45 Suppl 4: IV1-IV11.
23. The French METAVIR Cooperative Study Group. Intraobserver and interobserver variations in liver biopsy interpretation in patients with chronic hepatitis C. Hepatology 1994; 20:15-20
24. Bedossa P., Poynard T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology 1996; 24:289-293
25. Knodell R.G., Ishak K.G., Black W.C., et al. Formulation and application of a numerical scoring system for assessing histological activity in asymptomatic chronic active hepatitis. Hepatology 1981; 1:431-435
26. Lok A.S., McMahon B.J. AASLD Practice Guidelines: Chronic Hepatitis B. Hepatology., 2007; 45:507-539.
27. Liaw Y.F., Leung N., Kao J.H., et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2008 update. Hepatol Int., 2008; 2:263-283.
28. Malik A.H., Lee W.M. Chronic hepatitis B virus infection: Treatment strategies for the next millennium. Ann Intern Med 2000; 132:723-31.
29. Lok A.S., McMahon B.J. Chronic hepatitis B. Hepatology 2007; 45:507-539.
30. Cooksley W.G. Treatment with interferons (including pegylated interferons) in patients with hepatitis B. Semin Liver Dis 2004; 24:45-53.
31. Perrillo R.P. Therapy of hepatitis B - viral suppression or eradication? Hepatology 2006; 43 (suppl 1):S182-S193.
32. Hoofnagle Jay H. and Di Bisceglie Adrian M. The Treatment of Chronic Viral Hepatitis. 1997; 336:347-356.
33. http://www.hcvadvocate.org/hcsp/hcsp_pdf/HBV%20Treatment%20Overview.pdf as accessed in July 2009.
34. www.gilead.com/pdf/viread_pi.pdf as accessed in July 2009.
35. B-mmel Florian van and Berg Thomas. Role of tenofovir in the treatment of chronic HBV infection. Future Virol. 2008; 3 (3):207-220.
36. Ray A.S., Myrick F., Vela J. E., Olson L.Y., Eisenberg E. J., Borroto-Esodo K., Miller M. D., and Fridland A., 2005. Lack of a metabolic and antiviral drug interaction between tenofovir, abacavir and lamivudine. Antivir. Ther. 10:451-457.
37. Delaney William E., IV,* Ray Adrian S., et al. Intracellular Metabolism and In Vitro Activity of Tenofovir against Hepatitis B Virus Antimicrob. Agents Chemother. 2006; 7: 2471-2477
38. Xiong X., Yang H., Westland C.E., Zou R., and Gibbs C.S., 2000. In vitro evaluation of hepatitis B virus polymerase mutations associated with famciclovir resistance. Hepatology 31:219-224.
39. Xiong X., Flores C., Yang H., Toole J.J., and Gibbs C.S., 1998. Mutations in hepatitis B DNA polymerase associated with resistance to lamivudine do not confer resistance to adefovir in vitro. Hepatology 28:1669-1673.
40. http://www.accessdata.fda.gov/drugsatfda_docs/label/2008/021356s026lbl.pdf as accessed in July 2009.
41. Yang H., Qi X., Sabogal A., Miller M. D., Xiong S., and Delaney W. E., IV. 2005. Cross-resistance testing of next- generation nucleoside and nucleotide analogs against lamivudine-resistant HBV. Antivir. Ther. 10:625-633.
42. Brunelle M. N., Jacquard A. C., Pichoud C., Durantel D., Carrouee-Durantel S., Villeneuve J. P., Trepo C., and Zoulim F. , 2005. Susceptibility to antivirals of a human HBV strain with mutations conferring resistance to both lamivudine and adefovir. Hepatology 41:1391-1398.
43. Telbivudine, a nucleoside analog inhibitor of HBV polymerase, has a different in vitro cross-resistance profile than the nucleotide analog inhibitors, adefovir and tenofovir. Antiviral research. 2009; 81:147-155.
44. Selection of an entecavir-resistant mutant despite prolonged hepatitis B virus DNA suppression, in a chronic hepatitis B patient with pre-existent lamivudine resistance: Successful rescue therapy with tenofovir. European Journal of Gastroenterology & Hepatology 20 (8):773-777, August 2008.
45. Menne Stephan, Cote Paul J., Korba Brent E., et al. Antiviral Effect of Oral Administration of Tenofovir Disoproxil Fumarate in Woodchucks with Chronic Woodchuck Hepatitis Virus Infection . Antimicrobial Agents and Chemotherapy, 2005; 49:2720-2728.
46. Heijtink R.A., Kruining J., de Wilde G.A., Balzarini J., De Clercq E., Schalm S.W. Inhibitory effects of acyclic nucleoside phosphonates on human hepatitis B virus and duck hepatitis B virus infections in tissue culture. Antimicrob Agents Chemother 1994 Sep; 38 (9):2180-2.
47. Treatment with Tenofovir for 96 Weeks Results in High Rate of HBV DNA Suppression in Patients with HBeAg- NegativeChroniChronic Hepatitis BVInfection. http://www.clinicaloptions.com/Hepatitis/Conference%20Coverage/AASLD% 20 2008/Tracks/Approved%20HBV%20Agents/Capsules/146.aspx. accessed in June 2009.
48. Marcellin P., Buti M., Krastev Z., et al. Two-year tenofovir disoproxil fumarate (TDF) treatment and adefovir dipivoxil (ADV) switch data in HBeAg-negative patients with chronic hepatitis B (study 102), preliminary analysis. Program and abstracts of the 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31-November 4, 2008; San Francisco, California. Abstract 146.
49. Tenofovir Provides Effective and Sustained Virologic Suppression in HBeAg-Positive HBV-Infected Patients Through 96 Weeks.http://www.clinicaloptions.com/Hepatitis/Conference%20Coverage/AASLD%202008/Tracks/Approved%20HBV%20Agents/Capsules/158.aspx. accessed in June 2009.
50. Heathcote E., Gane E.J., de Man R.A., et al. Two-year tenofovir disoproxil fumarate (TDF) treatment and adefovir dipivoxil (ADV) switch data in HBeAg-positive patients with chronic hepatitis B (Study 103), preliminary analysis. Program and abstracts of the 59th Annual Meeting of the American Association for the Study of Liver Diseases; October 31-November 4, 2008; San Francisco, California. Abstract 158.
51. Van Bommel F., Wunsche T., Mauss S., et al. Comparison of Adefovir and Tenofovir in the treatment of lamivudine-resistant hepatitis B virus infection. Hepatology.2004; 40:1421-1425.
52. Tenofovir for Patients with Lamivudine-Resistant Hepatitis B Virus (HBV) Infection and High HBV DNA Level during Adefovir Therapy. Hepatology 2006; 44: 318-325.
53. Buti M., Hadziyannis S., Mathurin P., et al. i. Tenofovir disoproxil fumarate (TDF) is highly active for treatment of chronic hepatitis B in subjects with cirrhosis. 43rd annual meeting of the European Association for the Study of the Liver (EASL 2008). Milan, Italy. April 23-27, 2008. ii.Two-years safety and efficacy of tenofovir disoproxil fumarate (TDF) in patients with HBV-induced cirrhosis. Program and abstracts of the 44th Annual Meeting of the European Association for the Study of the Liver; April 22-26, 2009; Copenhagen, Denmark. Abstract 21
. 54. Case Report Successful Rescue Therapy with Tenofovir in a Patient with Hepatic Decompensation and Adefovir-Resistant HBV Mutant. Comparative Hepatology 2006, 5:1.
55. Neff G.W., Nery J., Lau D.T.Y., et al. Tenofovir Therapy for Lamivudine Resistance Following Liver Transplantation. Ann Pharmacother 2004; 38:1999-2004.
56. Terrault Norah A. Benefits and Risks of Combination Therapy for Hepatitis B. HEPATOLOGY 2009; 49:S122-S128.
57. Effect of switching to tenofovir with emtricitabine in patients with chronic hepatitis B failing to respond to an adefovir-containing regimen. Eur J Gastroenterol Hepatol. 18:1247-1253.
58. Marcellin P, Heathcote E J, Jacobson I, et al. Safety and Tolerability of 96 Weeks of Tenofovir Disoproxil Fumarate (TDF) Treatment in HBeAg-Negative and -Positive Patients Infected with Chronic Hepatitis B (Chronic Hepatitis B); 44th Annual Meeting of the European Association for the Study of the Liver; April 22-26, 2009; Copenhagen, Denmark.
59. Manns M., Jeffers L., Dalekos G., et al. The Antiviral Response To Tenofovir Disoproxil Fumarate (TDF) is Comparable in Lamivudine (LAM)-Na-ve and LAM-Experienced Subjects Treated for Chronic Hepatitis B (Chronic Hepatitis B) presented at EASL 2008 (#1587).
60. Review: Current status of antiviral therapy for hepatitis B. Therapeutic Advances in Gastroenterology 2008; 1; 61
61. Dusheiko B. G., Antonakopoulos N. Current treatment of hepatitis. Gut 2008; 57:105-124.
62. Lai C.L., Gane E., Liaw Y.F., et al. Telbivudine versus lamivudine in patients with chronic hepatitis B. N Engl J Med 2007;357:2576-88.
63. Seifer M., Patty A., Serra I., Li B., Standring D.N. Telbivudine, a nucleoside analog inhibitor of HBV polymerase, has a different in vitro cross-resistance profile than the nucleotide analog inhibitors, adefovir and tenofovir. Antiviral Res., 2009; 81:147-155.
64. Liaw Y.F., Gane E., Leung N., et al. 2-Year GLOBE trial results: Telbivudine is superior to lamivudine in patients with chronic hepatitis B. Gastroenterology 2009; 136:486-495.
65. European Association for the Study of the Liver. Journal of Hepatology.2009; 50 227-242.
Related Topics
More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items

28 Jul, 26
Journal Scans
28 Jul, 26

28 Jul, 26
Journal Scans
27 Jul, 26

27 Jul, 26


