Postpartum Haemorrhage
A Comprehensive Approach
AMTSL is an effective measure to prevent PPH. It can be provided by trained health-care providers linked to essential supplies, wherever a woman is giving birth, including at home. AMTSL speeds up delivery of the placenta by increasing the uterine contractions and prevents PPH by averting uterine atony.
The three components of AMTSL are as follows:
- Administration of a uterotonic agent within one minute after the baby is born.
- After the cord is clamped, delivery of the placenta by a CCT (gently pulling on the umbilical cord) with counter-traction on the fundus.
- Fundal massage after the delivery of the placenta.
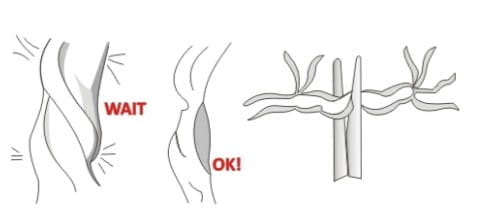
Previous data recommended early cord clamping for quicker separation of the placenta.
Later on, the WHO recommended late cord clamping, i.e., waiting either for 2 to 3 minutes or for the cord pulsations to stop. Late cord clamping helps improve haemoglobin concentration in the newborn and is associated with a reduced incidence of intraventricular haemorrhage.
Immediate cord clamping after childbirth is no longer a component of AMTSL.
The ideal way is to prevent PPH, rather than to treat it. It is said that 70 - 80% cases of PPH are due to uterine atony and can be prevented by AMTSL. And though it is a simple three-step procedure, it is not followed efficiently.
Once the exact cause of PPH is identified, it can be managed medically or surgically. All the four uterotonics can be used, but a higher dose may be required, sutures may be needed to be placed if direct pressure does not stop the bleeding, evaluation of coagulation status and replacing appropriate blood components may also be required.
It is necessary to wait for the uterine contraction before a CCT, but signs of placental separation such as a gush of blood are not necessary prior to instituting a CCT.
The steps for a CCT include the following;
- Start the CCT by first clamping and cutting the cord after cord pulsations have ceased or ∼2 to 3 minutes after the birth of the baby, whichever comes first. Place one clamp 4 cm from the baby's abdomen.
- Gently milk the cord towards the woman's perineum and place a second clamp on the cord ∼2 cm from the first clamp. Cut the cord using sterile scissors and tie the cord. Hold the cord close to the perineum using a clamp.

- Place the palm of other hand on the lower abdomen just above the woman's pubic bone to assess for uterine contractions. If a clamp is not available, the CCT can be applied by encircling the cord around the hand.

- Do the CCT only when there is a contraction. With the hand just above the pubic bone, apply external pressure on the uterus in an upward direction (towards the woman's head). At the same time, with the other hand, pull with firm, steady tension on the cord in a downward direction. AVOID jerky or forceful pulling.
- If the placenta does not descend during the 30 - 40 seconds of the CCT, (i.e. there are no signs of placental separation), do not continue to pull on the cord. Gently hold the cord and wait until the uterus is well contracted again. With the next contraction, repeat the CCT with counter-traction.
- Do not release the support on the uterus until the placenta is visible at the vulva. Deliver the placenta slowly and support it with both hands.

- As the placenta is delivered, hold and gently turn it with both hands until the membranes are twisted. Slowly pull to complete the delivery. If the membranes tear, examine the upper vagina and cervix to remove any pieces of remaining membrane.

AMTSL is associated with a slightly increased risk of retained placenta; however, this is more than compensated by the significantly decreased incidence of PPH and shortening of the third stage of labour.
Given orally, misoprostol has a faster onset of action. The POPPHI has documented that oral misoprostol acts within 3 to 5 minutes, peaks between 18 and 34 minutes and the effect lasts for 75 minutes.
In a pharmacokinetics study, oral misoprostol was detected at 7.5 minutes and peaked between 7.5 and 30 minutes. The serum concentration of rectal misoprostol, on the other hand, rose gradually, reached a maximum level between 15 and 60 minutes and declined slowly. Rectal misoprostol has a slower onset of action but longer duration of action.
Another study showed that the duration of action of misoprostol ranges from 1.5 hours when given orally to 4 hours when given rectally.
In a case when both quick onset and prolonged duration of action is required, a combination of oral and rectal misoprostol can be used.
Both the routes have been found to be very effective in reducing PPH. Though oral route is the approved one, the rectal route is also commonly used.
In case quick onset of action is required, oral misoprostol can be used. This may be of clinical significance in PPH treatment.
Rectal misoprostol is associated with a longer duration of action. This long half-life could prolong the uterine contraction, thus preventing a delayed haemorrhage. In case prolonged duration of action is required, rectal misoprostol can be used.
In a case when both quick onset and prolonged duration of action is required, a combination of oral and rectal misoprostol can be used.
The occurrence of shivering and elevated temperature with misoprostol may be related to the PGE1 effect on the central thermoregulatory centers. While misoprostol is associated with an increase in shivering, it is generally regarded as a nuisance rather than a serious morbidity.
Side effects of misoprostol on the mothers are transient and in the study that compared misoprostol with placebo, there was no evidence of adverse effects on the neonates whose mothers were given misoprostol.
Shivering is a common, transient side effect associated with misoprostol that is not life-threatening and, in most cases, it does not need any treatment. However, a very small proportion of women require treatment to alleviate it, and this effect can be easily managed by the delivery room staff.
Paracetamol (oral/I.V.) can be used to manage this side effect. Other NSAIDs should NOT be used.
It can also be easily treated with an antihistamine such as chlorpheniramine. In rare and worst cases not responding to any treatment, steroids (e.g., hydrocortisone 100 mg I.V. stat) can be used.
Diarrhoea is a side effect more commonly seen with PGF2#945; (carboprost). The most common and transient side effects associated with misoprostol are pyrexia and shivering. In case diarrhoea is a concern, misoprostol can be given orally.
In some cases, the body temperature may rise more than 100 °F.
No. Misoprostol is, in fact, used to prevent PPH arising due to an atonic uterus.
Paracetamol, and not NSAIDs, is given to manage pyrexia and shivering related to misoprostol.
Anaphylactic reactions can occur with all drugs, even with water. But these are very rare with misoprostol and there is no reason to worry about anaphylactic reactions when using misoprostol.
Generally, if facilities are available for a caesarean section, then there would be facilities for administering an injectable uterotonic too.
Still, if required, there are many studies proving the effectiveness of misoprostol when used in caesarean deliveries too. Here, it has been used in dosages ranging from 400 to 1,000 mcg via the oral, buccal, sublingual and rectal routes. Misoprostol, when used alone in caesarean section deliveries, has been found to be as effective as or more effective than oxytocin. When used in combination with oxytocin, it was more effective than oxytocin alone.
Earlier when misoprostol was not approved, oxytocin, methylergometrine and carboprost were the uterotonics that were used for PPH management.
But the use of these uterotonics is not feasible in the developing world where deliveries still take place in rural areas with untrained birth attendants. Injectable uterotonics are unstable in high temperatures and require cold-chain storage. They also require skills that birth attendants who do not practice AMTSL might not possess.
Of all the uterotonics, methylergometrine is contraindicated in females with cardiac disorders (since it increases the BP) and carboprost is contraindicated in females with cardiac, pulmonary, hepatic and renal disorders. Apart from these contraindications, methylergometrine and carboprost are also associated with serious side effects like hypertension and bronchospasm.
The approval of misoprostol has been more of a boon in gynaecology and obstetrics, and is used extensively for PPH management.
Misoprostol and oxytocin are the only uterotonics that have no known contraindications and can be used even when the birth attendant is not fully aware of the patient's condition.
When misoprostol 600 mcg was not available as a single tablet, three tablets of misoprostol 200 mcg were used for the prevention of PPH. Hence, even now, in case misoprostol 600 is not available, three tablets of misoprostol 200 mcg can be used without compromising the effectiveness. But using a single tablet of MISOPROST 600 is more convenient for the doctor and the attending paramedic staff.
Yes. Misoprostol, in the dose of 600 mcg, has been approved by the DCGI to be used for the prevention of PPH and, hence, can be used prophylactically. Misoprostol tablets are approved to be given orally, but may be administered rectally too. For prevention, the 400-600 mcg dose is used; and a higher dose is used only if the bleeding is more.
For the therapeutic management of PPH, up to 1,000 mcg of misoprostol can be given.
Though misoprostol in the dose of 600 mcg is approved for oral use, all the routes of misoprostol, i.e., oral (400-600 mcg), sublingual (400-800 mcg) and rectal (600-1,000 mcg), are effective in reducing PPH. The vaginal route is the preferred route in the cases of abortion and cervical ripening, but it is NOT a recommended route of administration in cases of PPH as the bleeding would wash away vaginally-administered misoprostol before adequate absorption can take place.
Misoprostol 600 mcg orally for prevention of PPH is approved by the DCGI.
Yes. That is the first step in AMTSL - administration of 600 mcg misoprostol orally or sublingually after the birth of the baby. Administering a uterotonic drug within one minute of the baby's birth stimulates uterine contractions that will facilitate separation of the placenta from the uterine wall.
Misoprostol will minimize the third stage of labour and help expel the placenta quicker.
In such cases, another 400 mcg of misoprostol can be given (standard therapeutic dose of 1,000 mcg). Consideration should be given to concurrent use of other uterotonics. If need be, 400 mcg of misoprostol can be repeated every fourth hour up to a cumulative dose of 2,400 mcg per day.
Also, one has to keep in mind that alternative uterotonics and transferring to higher health-care facilities might be needed to be considered to rule out other aetiologies of PPH.
Yes. There is no contraindication for its use in PIH.The two uterotonics that cannot be used in this case are methylergometrine and carboprost. Oxytocin can also be used, but in a tropical country like ours, it has to be stored at 2-8°C for optimum efficacy. But if this injection is not stored properly (left out in the trays unattended), it may lead to 27% reduction in efficacy in one month.
Misoprostol, on the other hand, does not require special transport or storage requirements and can be stored for many years. Any therapeutic dose of misoprostol can be used; usually, 1,000 mcg may be used to treat PPH.
Yes. Misoprostol is safe to be used in asthmatics as it causes smooth muscle dilation, unlike PGF2α.
Yes. Rh-negative pregnancy is not a contraindication for misoprostol use. The concern in these cases is that the uterotonics cause a back-flow of the foetal blood into maternal circulation when the uterus contracts suddenly with open maternal sinuses. But administration of 300 mcg of Anti-D within 72 hours of delivery will take care of materno-foetal haemorrhage of upto 30 ml of blood.
Cord clamping may also be an issue - delayed cord clamping is done after the cord pulsations have stopped and because of this reason, blood would not be pushed into maternal circulation.
Misoprostol can be used for AMTSL irrespective of the drug used for induction.
Either route can be used; with both routes, the action starts within 3 to 5 minutes and peaks by 18 to 34 minutes. The rectal route should preferably be avoided in emergencies as it takes a longer time to act.
Either dose can be used. A single tablet ensures an adequate dose at one go, more convenience and is simpler as compared to multiple tablets.The approved dosage is 600 mcg orally in preventing PPH.
No, misoprostol has not been associated with increased incidence of retained placenta as against methylergometrine.
Misoprostol is a relatively new drug for managing PPH as compared to oxytocin / methylergometrine. It is only in the last few years that clinically viable robust data is available regarding its usefulness in preventing PPH. And now, the DCGl approval of misoprostol 600 mcg its use in the prevention of PPH has proved it to be a boon in obstetrics and gynaecology. Hence, the Cipla webcast was one such endeavour to popularize its use.
A combination of uterotonics can be used in situations where the bleeding does not respond to one uterotonic agent. However, routine use of all the uterotonics is not usually necessary - it increases the cost of care while adding the unnecessary risks of drug side effects.
Misoprostol is very stable in vitro. It has been shown to retain its potency even two years after being exposed to light at typical room temperatures. This gives it an inherent advantage over the other uterotonics, which have stringent storage criteria, especially in low-resource settings. However, it should be stored in a dry place.
Uterine packing entails placing, carefully and systematically, several yards of gauze inside the uterine cavity to occlude the whole intrauterine space and, thus, control major haemorrhage. The technique fell out of favour in the 1950s, as it was thought to conceal haemorrhage and cause infection. It re-emerged in the 1980s and 1990s after these concerns were not verified.
The main disadvantages of this technique are as follows:
- Experience is required to pack properly and tightly and, therefore, junior residents may not be able to perform proficiently, especially if they have large hands. Speed is also necessary because the intrauterine/vaginal hand becomes numb rapidly.
- Delay in recognizing continual haemorrhage as the blood needs to soak through yards of gauze before it becomes evident.
- Success of the procedure will not be known immediately, as the blood must soak through the pack to reveal itself.
- The tightness of the pack is difficult to determine, especially if the blood soaks through, leading to a loss of the tamponade effect.
- Potential risk of trauma and infection.
- Removing the pack may often require a separate surgical procedure to dilate and extract the intrauterine material, thus falling short of an ideal option.
Notwithstanding, uterine packing remains an option in certain cases, e.g., where medical management has not controlled the bleeding and surgical management cannot be undertaken immediately; balloon catheters are not available; referring a patient with ongoing haemorrhage; patient is in coagulopathy, and blood products are not immediately available.
The risk of intrauterine infection can be minimized by prophylactic antibiotics.
Nipple stimulation and breastfeeding do not stimulate the release of enough oxytocin to cause significant uterine contraction.
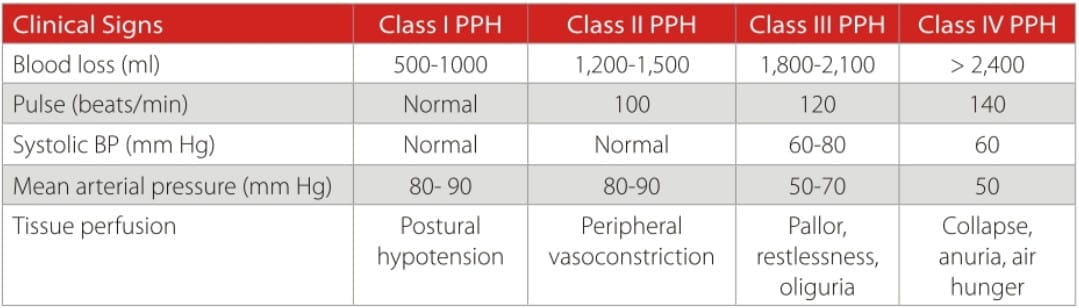
The combined blood loss in the third and fourth stage of labour is 500 - 1,000 ml; though this is an average range and not an absolute value. Blood loss of 250 ml with haemoglobin of 5 mg/dl also calls for treatment as in excessive blood loss.
The sample size depends on prevalence of PPH in the region where the trial is going to be carried out and on the number of patients that can be enrolled. To arrive at a statistically significant result, a sample size of at least 100 patients would be required.
Surgical techniques are generally used for the treatment of PPH, rather than its prevention.
B-Tynch Suture
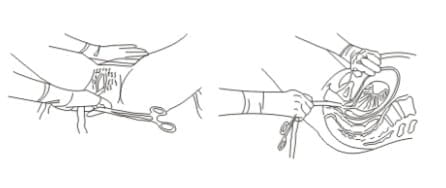
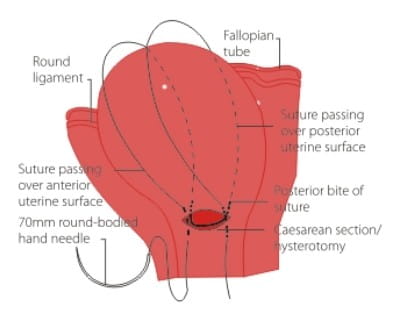
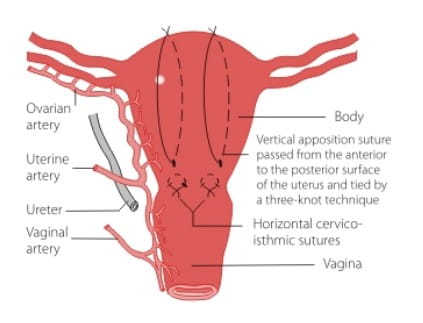
The B-Lynch suture aims to exert continuous vertical compression on the uterine vascular system. Laparotomy, uterine exteriorization and an opened uterine cavity are necessary. The potential efficacy of the B-Lynch suture should be tested by performing an open bimanual compression to see whether the bleeding stops, before proceeding to place the suture into the uterus. If the bleeding stops on applying such compression, there is a good chance that application of the B-Lynch suture will stop the bleeding.
Vertical Uterine Compression Sutures
These are an alternative to the B-Lynch technique if no lower segment caesarean incision is present. They may be placed without opening the uterus, using a straight 10 cm needle. Ensure downward bladder retraction and place two to four vertical sutures. Check that the compression sutures have worked by observing the blood loss per vaginum before closing the abdomen.
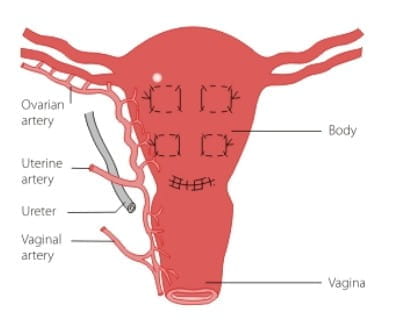
CHO Multiple Square Compression Sutures
Multiple square sutures are used to cover the whole body of the uterus and may be useful in cases of placenta previa (make sure to leave a drainage portal). Check that the compression sutures have worked by observing the blood loss vaginally before closing the abdomen. Suture through with a straight 10 cm needle.
Stepwise Devasculorization
This surgical approach starts with ligature of the uterine artery and its distribution to the uterus, either unilaterally or bilaterally, preferably as it emerges from crossing over the ureter or as it approaches the uterine wall to penetrate and establish its divisions and the infundibulo pelvic vessels before it enters the uterus.
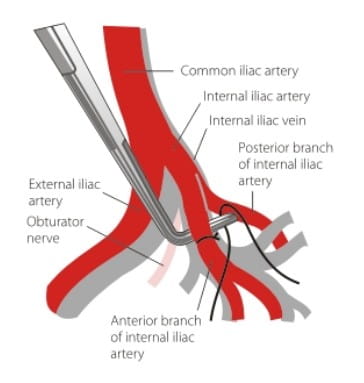
Internal Iliac Artery Ligation
Conditions indicating ligation are:
- PPH due to atonic uterus refractory to other measures.
- Abruptio placentae with uterine atony.
- Abdominal pregnancy with pelvic implantation of the placenta.
- Placenta accrete.
Therapeutic indications include the following:
- Before or after hysterectomy for PPH.
- Continuous bleeding from the broad ligament base.
- Profuse bleeding from the pelvic side wall or the angle of the vagina.
- Diffuse bleeding without a clearly identifiable vascular bed.
- Ruptured uterus in which the uterine artery may be torn at its origin from the internal iliac artery.
- Where extensive lacerations of the cervix have occurred following difficult instrumental delivery.
Hysterectomy
Emergency peripartum hysterectomy is the best option when uterine atony is unresponsive to uterotonics, where facilities for embolization are not available, and/or the obstetrician is not well-versed with conservative surgical procedures. Uterine rupture secondary to obstructed labour and a previous caesarean section may be other indications. If the rupture is extensive and the haemorrhage cannot be contained by suture of the ruptured area, then a hysterectomy may be necessary.
Tranexamic acid, being an anti-fibrinolytic, is going to prevent bleeding. Systemic anti-fibrinolytic agents are widely used in surgery to prevent fibrinolysis in order to reduce surgical blood loss.
Use of tranexamic acid for managing PPH is not evidence-based and, in practice, it is used only when blood loss is not controlled adequately with the uterotonics. In this case, platelets and FFPs are given and tranexamic acid is given as an add-on. It may only be useful in cases of generalized oozing from the tissues as a result of coagulopathy rather than in cases of gross uterine atony and active PPH. It is a supportive rather than an active therapy.
A systematic review was conducted to assess the effectiveness and safety of anti-fibrinolytic agents in post partum bleeding.The administration of tranexamic acid was associated with a reduction in blood loss by 92 ml. The most frequently reported adverse effect of tranexamic acid was nausea, although the increase was easily compatible with the play of chance. It was concluded that tranexamic acid may reduce blood loss in PPH.
The classification of the haemorrhage can be based on a physiological response to the loss of circulating blood volume.
Oxygen has no role in "prevention" of PPH; it is used as an adjunct during the management of excessive bleeding for maintaining adequate tissue perfusion and avoiding tissue hypoxia. Adequate tissue perfusion prevents lactic acidosis and helps better preservation of the tissue, thus avoiding multiple organ dysfunction.
In this case, early referral to a higher health care facility would be an ideal option for better management of PPH. Caesarean section and transfusion may have to be done. Combination of misoprostol and oxytocin may be required to manage the atonic PPH.
Availability of adequate FFPs / cryoprecipitate components is indeed necessary.
Hysterectomy, of course, results in infertility. But the surgical methods do not compromise future fertility. Vaginal deliveries have been reported after carrying out these procedures.
But two cases have been reported, one with B-Lynch and the other with Cho. In one patient, since the B-Lynch suture had cut through the uterine wall, there was uterine wall deficiency, which would affect future fertility. In another patient, Cho's square suture was related to pyometria.
But by and large, after uterine artery embolization, internal iliac artery ligation or devascularization, the uterus does not go through any ischaemic changes.
Any suture that goes through the uterine cavity has got a chance of producing Asherman syndrome. Local tissue necrosis is one possibility and collection of material near the suture is another possibility. Hence, Asherman syndrome can occur, but should not be considered a major problem.
If there is a patient with placenta previa accreta not bleeding at the time of surgery and caesarean section has been done, it is advisable not to induce bleeding by plucking the pieces of placenta. If it is not true accrete; it may separate by itself. If the placenta doesn't separate, it is advisable not to do anything, close and give methotrexate. Case reports have shown that everything was normal after a period of six months.
Published data have used dilatation and curettage, uterine artery embolization with or without methotrexate, tamping B-lynch suture, singly with methotrexate, and mifepristone and caesarean hysterectomy for the management of placenta accreta.
In most places, with the help of sonologists, this condition can be picked up well before the delivery.
The relation of the FFP does not depend only on the INR. It depends on the overall coagulation profile, including the platelet count, PCT, etc. which has to be taken into consideration. One thing that has to be kept in mind is that it would suffice if the INR stays below 2, preferably around 1.5 in a patient with DIC.
Oxytocin injection is usually administered I.M. after the delivery of the anterior shoulder, or at the latest, immediately after delivery of the child. It may also be administered by a slow I.V. drip. I.V. methylergometrine is contraindicated in view of its sudden vasoconstrictive actions, leading to a precipitate rise in the BP. Oxytocin plus methylergometrine injection has to be administered I.M. It may also be administered as an I.V. injection, but this route of administration is generally not recommended.
Timely identification of PPH will not result in shock and majority of cases with atonic haemorrhage will respond to PGs and oxytocin. However if the PPH is unresponsive to medical management, the next option is surgical management. Balloon uterine tamponade or uterine packing can be an option while awaiting arrangements for surgery or during transportation to a tertiary care institute.
Waiting for the uterine tone to return despite conventional means while there is ongoing haemorrhage can be counterproductive. So, if there is a suspicion of inadequate response with medical management, move over to surgical management as soon as possible. If conservative surgery has not controlled bleeding, a decision for a hysterectomy should be taken early rather than late, because by the time the next decision is taken, the patient might already be exsanguinated.
Rather than the choice of surgery, an experienced obstetrician should be present while managing the PPH surgically. For decreasing the time taken for a caesarean, the Misgav-Ladach method can be used.
Ideally, methylergometrine is NOT given I.V. It should be given I.M. to avoid a precipitous rise in the BP. Its routine use for the AMTSL has been shown to increase the risk of retained placenta and manual removal of placenta.
Conservative management includes medical management with one or more of the uterotonics - oxytocin, misoprostol, carboprost, methylergometrine.
Conservative surgery methods include stepwise devascularization of the uterus, B-Lynch suture, Haymans suture, the Cho multiple square method, etc.
No studies with adequate subjects document the effectiveness of cord drainage.
AMTSL remains the simple, effective and recommended tool for the prevention of PPH.
This technique involves collecting a patient's blood (2-4 units) into anticoagulant-containing storage bags at the outset of surgery, accompanied by I.V. replacement with crystalloids or colloids to maintain normovolemia. The patient's whole blood can then be transfused later, in case, as needed.
Use of cell salvage in obstetrics is classically contraindicated; however, little data is available to substantiate this contraindication. This contraindication arises from a fear that shed blood can be contaminated with amniotic fluid, and re-administration may lead to an iatrogenic amniotic fluid embolism, though, significant data exist to support the use of cell salvage in obstetrics. Despite the reassuring data, several precautions should be taken when salvaging blood in obstetrics.
First, minimizing the aspiration of amniotic fluid through a double suction set-up is advisable. One suction should be connected to the cell salvage reservoir and used for suctioning of the blood. The other should be connected to the regular wall suction and used only for aspiration of the amniotic fluid. In this way, the volume of amniotic fluid contamination is minimized.
Secondly, the utilization of leucocyte reduction filters at the completion of the processing can reduce the foetal squamous cell contamination to a level comparable to maternal blood contamination. These filters should be used by the anaesthesiologist with a pressure of <300 mm Hg being placed on the reinfusion bag.
Lastly, foetal red cell contamination is present. An Rh incompatibility between the mother and the infant may suggest that the Anti-D dose following delivery may need to be modified.
The evidence on the overall efficacy of autologous normovolaemic haemodilution is conflicting with respect to blood savings and transfusion avoidance, but it appears to be safe and efficacious in centers that make routine use of this technique.
Misoprostol acts by inducing uterine contractions and restoring uterine tone. It is indicated for the prevention and treatment of atonic PPH. It is not useful in cases of PPH secondary to coagulopathy. Transfusion of FFP/ cryoprecipitate/platelets, depending upon the coagulation profile, would be the ideal management in these cases.
Yes, it is available; however, it is quite costly (NovoSeven is available in India, approximately Rs. 35,000 and Rs. 75,000 for 1.2 mg and 2.4 mg vials, respectively).
- Routine AMTSL should be practiced.
- Early recognition and appropriate management / referral should be made.
- All set-ups should have a "PPH protocol" to be followed in emergency situations.
Electrolyte imbalance / dehydration rarely cause atonic PPH; however, these can adversely affect the outcome of individual cases of PPH. Proper management of labour, including adequate hydration and use of a partogram to avoid prolonged and obstructed labours, can help avoid these complications.
Haemostatic agents and vitamin K are likely to be of use in cases of coagulation disorders/ generalized oozing at surgery. However, they surely are not the first line drugs for PPH management, with its most common cause being uterine atony followed by tissue trauma.
Intramyometrial carboprost is effective, especially in cases of shock, wherein the I.M. dose might not be absorbed well due to inadequate perfusion.
With regards to intramyometrial vasopressin, there is no data to recommend such a practice.
AMTSL: Active Management of the Third Stage of Labour
BP: Blood Pressure
CCT: Controlled Cord Traction
DCGI: Drug Controller General of India
DIC: Disseminated Intravascular Coagulopathy
FFP: Fresh Frozen Plasma
I.M.: Intramuscular / Intramuscularly
I.V.: Intravenous / Intravenously
INR: International Normalized Ratio
NSAIDs: Non-Steroidal Anti-Inflammatory Drugs
PPH: Postpartum Haemorrhage
POPPHI: The Prevention of Postpartum Haemorrhage Initiative
PG: Prostaglandin
PIH: Pregnancy Induced Hypertension
PCT: Prothrombin Consumption Time
PGE1: Prostaglandin E1 analogue
PGF2 : Prostaglandin F2 analogue
WHO: World Health Organization
Reference:
Question and Answer Session after Webcast titled "PPH – Prevention is Easier than Cure", in November 2010; Speakers: Dr. Hema Divakar, Dr. Prakash Mehta & Dr. Ajay Dhawle.