Haemostasis for Postpartum Haemorrhage
Postpartum haemorrhage (PPH) refers to an estimated blood loss in excess of 500 ml following a vaginal birth and a loss greater than 1000 ml during a caesarean section.
These values are arbitrary as visual estimation of blood loss is not reliable. Patients with a low body mass index have a lower blood volume of 70 ml/kg and anaemic women have fewer reserves to withstand blood loss and hence will decompensate sooner.
PPH is commonly due to one or a combination of four processes referred to in the '4Ts' mnemonic:
- Tone (post-delivery poor uterine contraction)
- Tissue (blood clots and/or retained products of conception)
- Trauma (genital tract)
- Thrombin (coagulation abnormalities)
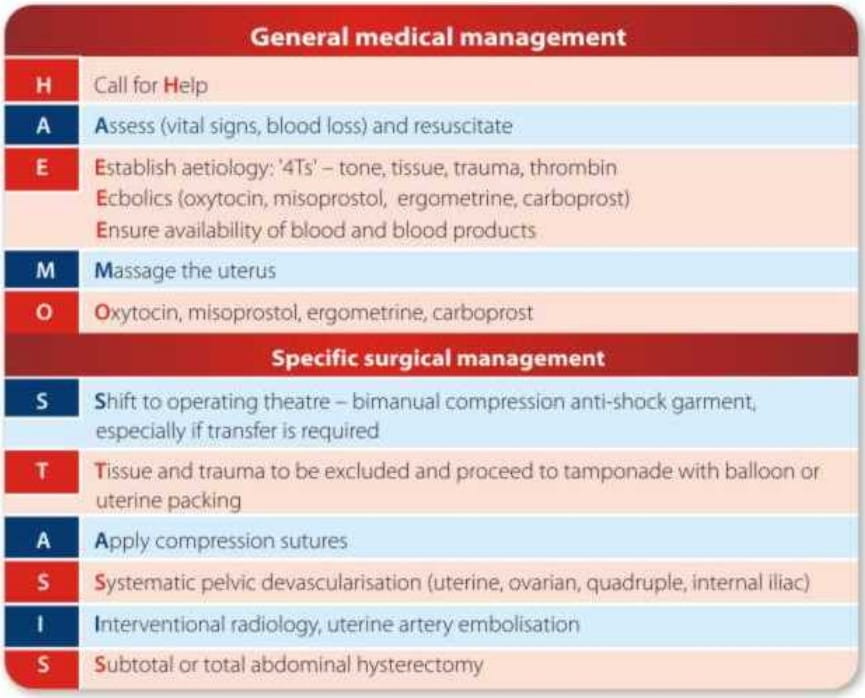
A management algorithm - HAEMOSTASIS - has been proposed to aid stepwise management of atonic PPH.
Major PPH must be managed appropriately by a multidisciplinary team -consultant obstetricians, anaesthetists, haematologists, midwives, theatre staff, blood bank, hospital staff and the intensive care unit staff should be alerted.
The components in the management of PPH are early recognition, prompt resuscitation and restoration of the circulating blood volume.
General resuscitation measures include assessment of the haemodynamic status by monitoring the patient's vital parameters - level of consciousness, blood pressure, pulse and oxygen saturation.
Accurate estimation of the blood loss warns of impending haemorrhagic shock. Different methods of estimation have been evaluated and guidelines to improve accuracy of the visual estimation of blood loss have been suggested.
Fluid resuscitation in PPH is often conservative because of underestimation of blood volume and rapid blood loss. It is important to remember that symptoms of hypovolaemia are often delayed due to compensatory mechanisms as the women are fit and young.
A loss of 1 L of blood requires replacement with 4-5 L of crystalloid (0.9% normal saline or lactated Ringer's solution) or colloids until cross-matched blood is made available, as most of the intravenous fluid shifts from the intravascular to the interstitial space.
As more time passes between the onset of severe shock and effective resuscitation, the chances of survival decrease because metabolic acidosis sets in.
The 'golden first hour' is the time at which resuscitation must be commenced to ensure the best chance of survival. The probability of survival decreases sharply after the first hour if the patient is not effectively resuscitated.
For the general acute management of PPH a 'rule of 30' has been proposed .The patient is most likely to have lost at least 30% of her blood volume and is in moderate shock leading to severe shock if her:
- Systolic BP falls by 30 mmHg,
- Heart rate rises by 30 beats/min,
- Respiratory rate increases to >30 breaths/min, and
- Haemoglobin or
- haematocrit drop by 30%, and/or
- Urinary output is<30 ml/hour.
- Tone- Thorough assessment of the uterine tone followed by administration of uterotonics and uterine massage if the uterus is atonic.
- Tissue - Exploration of the uterine cavity under anaesthesia to exclude or remove retained placental tissue and membranes.
- Trauma - If bleeding persists despite a well-contracted uterus, under anaesthesia, check for cervical tears or tears in the vaginal vault, as these may involve the uterus and/or broad ligament and may be the cause of retroperitoneal haematomas.
- Thrombin - If retained tissue or trauma is excluded and bleeding continues despite a well-contracted uterus, suspect a coagulation defect
Medical management of uterine atony, the most common cause of PPH, consists of oxytocin, ergometrine, misoprostol and carboprost.
Blood transfusion must be commenced if the estimated blood loss is over 30% of the blood volume or if the patient is haemodynamically unstable despite aggressive resuscitation. O negative blood should be transfused until grouped and cross-matched blood is available. Fresh frozen plasma, platelets, cryoprecipitate and other clotting factors (VIII, XIII, von Willebrand factor) may be required.
Bimanual uterine massage (vaginal hand in the anterior fornix and abdominal hand on the uterine fundus) is a very effective measure and reduces bleeding even if the uterus remains atonic, allowing resuscitation to be effective and, thus, reducing further blood loss.
Oxytocin - Oxytocin can be given as a slow IV bolus or as an infusion in order to maintain uterine contraction. Administered 10 IU intramuscularly, it acts within 2 to 3 minutes and the effect lasts about 15 to 30 minutes. There are no absolute contraindications, but an anti-diuretic effect with volume overload can develop with high cumulative doses. If the uterus remains atonic after initial oxytocic therapy, uterotonics can be repeated.
Ergometrine - Hypertension and cardiac disease are contraindications due to the possible development of severe hypertension and myocardial ischaemia.
Carboprost - Carboprost is a prostaglandin F2 analogue administered intramuscularly or intramyometrially. It is contraindicated in asthma (as it is bronchoconstrictive). Side effects include diarrhoea, vomiting, fever, headache and flushing.
Misoprostol - Misoprostol is a synthetic prostaglandin E1 analogue and has been used in the management of PPH. The dosage of misoprostol in prevention of PPH is 600 mcg given orally immediately after cord clamping.
Given orally, it acts within 3-5 minutes and has a moderately long sustained action of 75 minutes. As the peak serum concentration of oxytocin is much smaller than oral misoprostol, a combination of these two agents can provide a sustained uterotonic effect. Misoprostol does not require a syringe and needle, a skilled birth attendant trained and authorized for its administration. It does not require special transport or refrigeration and can be stored at room temperature
Recombinant activated factor VII may be an alternative haemostatic agent when the standard treatment is ineffective.
If conservative measures fail to control haemorrhage, surgical haemostasis should be commenced 'sooner rather than later'. All available interventions must be considered to stop haemorrhage including B-Lynch suture, uterine artery embolisation or even radical surgery.
In home births and primary / secondary health centres, transfer to a centre with greater facilities is indicated at this stage. A non-pneumatic anti-shock garment (NASG) can reverse the effect of shock on the body's blood distribution by applying external counter pressure to the legs and abdomen and returning blood to the vital organs, thus keeping the woman stabilised until she reaches a hospital. Its use could be critical in reducing maternal mortality in low-risk areas where reaching a health facility could take time.
Continuous bleeding indicates transfer to and evaluation in the operating theatre. Examination with appropriate lighting, equipment, analgesia and assistance permits assessment of the uterine tone and excludes retained tissue and trauma.
Uterine packing is considered effective, quick and safe procedure for controlling PPH.
Uterine balloon tamponade has been successfully used with a number of devices like Bakri balloon, condom Foley's catheter, Rusch urological hydrostatic balloon and Sengstaken-Blakemore oesophageal catheter. The early use of balloon tamponade results in reduced total blood loss and haemorrhage-related maternal mortality.
The 'tamponade test' arrests bleeding in most women with severe PPH and allows the obstetrician to identify women requiring a laparotomy. Some advantages are:
- Insertion is easy and rapid with minimal anaesthesia;
- It can be performed by relatively inexperienced personnel;
- Removal is painless; and
- Failed cases can be identified rapidly.
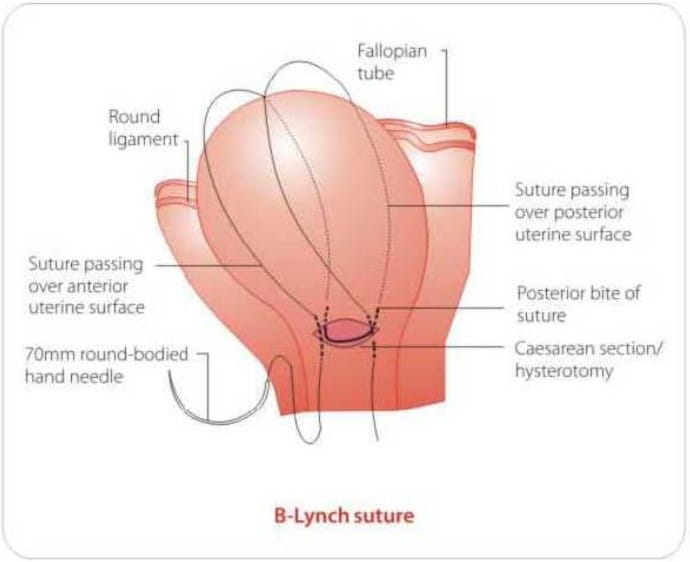
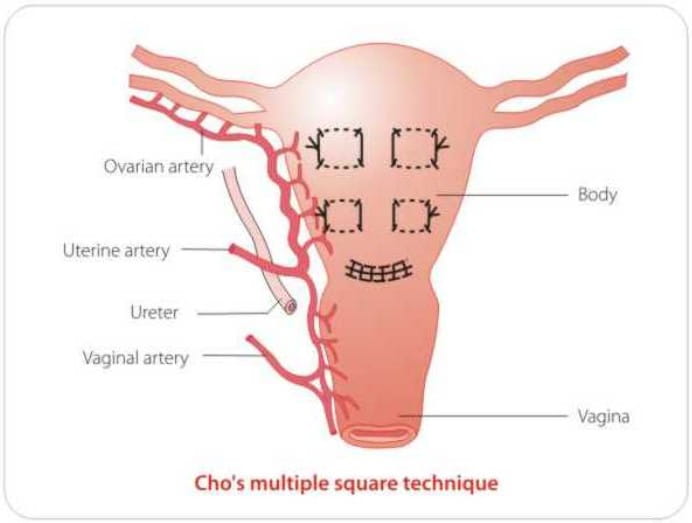
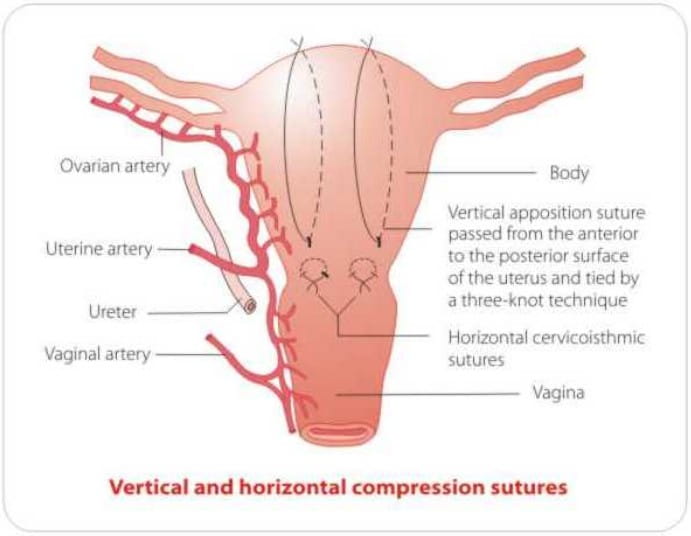
If the patient is stable and bimanual compression of the uterus has successfully achieved haemostasis, then compression sutures may be of value. Advantages are easy application of such sutures and preservation of fertility. Disadvantages the need for laparotomy. Recognised complications include erosion through the uterine wall, pyometra and uterine necrosis.
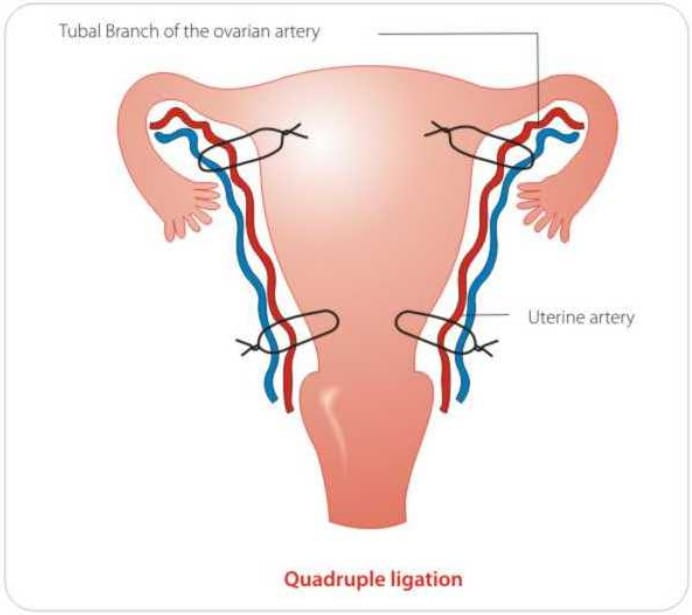
Pelvic devascularisation requires laparotomy, and progressive, step-wise devascularisation, whereby the uterine, ovarian and internal iliac arteries are ligated.
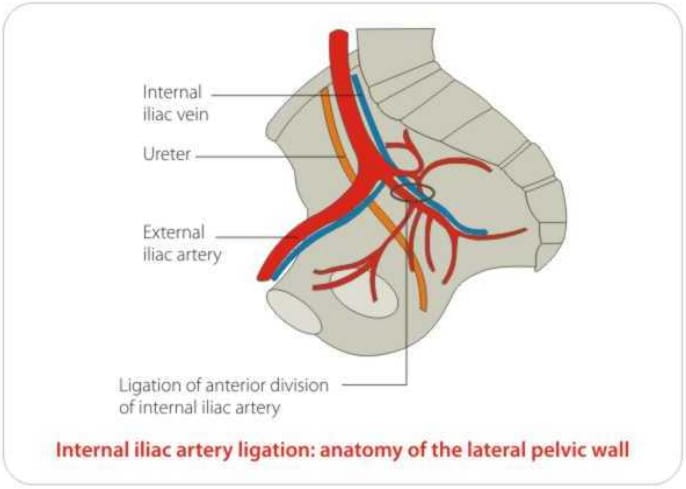
Internal iliac artery ligation is effective in arresting bleeding from within the genital tract, however,
- it takes time
- is technically challenging
- carries the risk of injury to neighbouring structures.
- a haemodynamically stable patient
- specialist surgical expertise
- a patient's desire to preserve her future fertility.
When arterial ligation fails, hysterectomy follows and has a higher morbidity compared with those patients undergoing hysterectomy without previous attempts at arterial ligation.
Arterial embolisation under fluoroscopic guidance has a success rate as high as 70-100% and the procedure has the potential to preserve fertility. Prophylactic embolisation has a role in an elective caesarean section when the placenta is thought to be morbidly adherent. Prerequisites are specialised equipment and an interventional radiologist with a great degree of expertise. Complications include haematoma formation, infection, contrast-related side effects and ischaemia, resulting in uterine and bladder necrosis.
Subtotal or total abdominal hysterectomy is usually a last resort in the management of PPH and must not be delayed if the conservative measures have failed to control it. Subtotal hysterectomy may not be effective when the source of the bleeding is in the lower segment, cervix or vaginal fornices.
Postoperative complications include bowel injury, fistula formation, pelvic haematoma, sepsis, urinary tract injury, vascular injury. The resultant loss of child-bearing and its psychological consequences must not be underestimated.
PPH is a major cause of maternal morbidity and mortality. Identification of risk factors antenatally and intra-partum is useful in the prevention and treatment of PPH. Rapid and prompt treatment measures should be instituted in a stepwise manner using the algorithm 'HAEMOSTASIS'. Protocols for the prevention and management of PPH should be constantly updated in every maternity unit.
1. Obstetrics, Gynaecology & Reproductive Medicine 2009; 19(5): 121 -126
2. www.path.org/files/MCHN_popphi_pph_uterotonic_trop.pdf