Furniture Induced Allergic Contact Dermatitis
An epidemic of severe dermatitis from chairs and sofas were noticed first in Finland and a few months later in the UK. Some patients reacted in patch tests (PTs) strongly to the material of their furniture, either leather or fabric. Clinical findings were very similar and unlike any known dermatosis. Many of these cases had been quite severe, resembling mycosis fungoides or septic infections, requiring hospitalization. The laboratory of Malmo University Dermatology Clinic helped to determine that material in sachets marked with 'mouldproof agent' were found to be used in sofas. These sachets contained dimethyl fumarate (DMF) which proved in skin tests to cause strong positive reactions.
Here, in this Top Digest we present four cases of furniture related dermatitis experienced in Finland and the UK.
History: A woman of 37 years, pregnant in her last trimester, was hospitalized in December 2006 for unknown infection and treated with intravenous antibiotics. Later it was determined that the infection was caused by a rash on her back and thighs. She gave birth 3 weeks prematurely. She was nursing the baby sitting a lot in a chair bought in November 2006.
Comment:The rash deteriorated and she received corticosteroid injections with some improvement. In February 2007, she read about the outbreak of other cases in Finland and contacted a dermatologist.
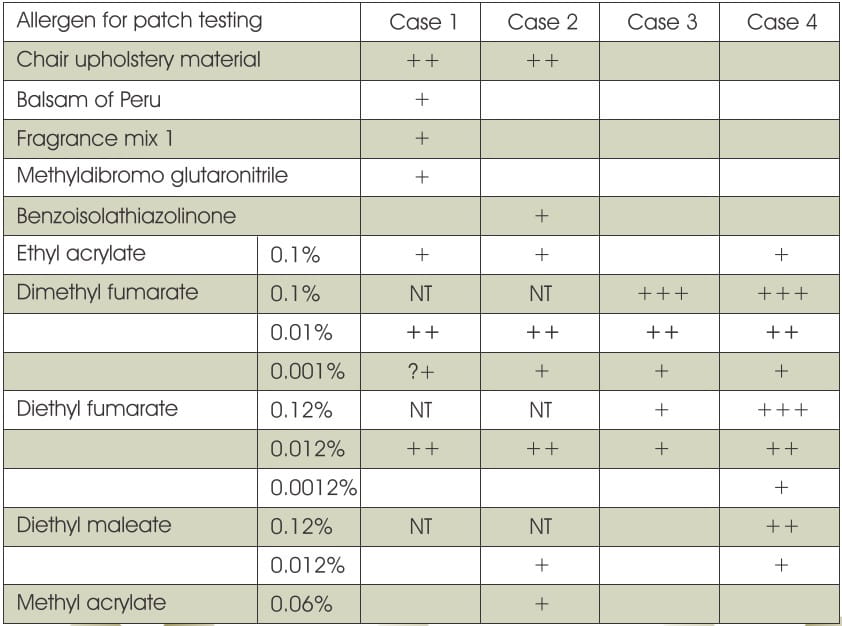
Patch test results are shown in Table 1.
History: A 45-year-old man with a mild psoriasis presented in December 2007 with a suspected flare. He had a severe oozing rash on his upper back.
Comment: When asked about a new chair, he admitted having occasionally sat on a new recliner chair during the past few weeks. The chair was removed immediately but his rash continued to flare for another 3-4 weeks before it subsided.
Patch test results are shown in Table 1.
History: A 43-year-old man was referred to the dermatologist for buttock dermatitis which had been treated by intravenous antibiotics.
Comment: He had bought a new leather suite approximately 10 weeks before his rash. The rash responded to potent topical steroids, and he has not experienced any skin problems since.
Patch test results are shown in Table 1
History: A 35-year-old lady presented with a 4 months history of a rash on her back and buttocks. Her partner had a similar less severe rash at the same time.
Comment: They had bought new leather suite 2 months before the onset of their symptoms. The rash improved with the use of topical steroids but had not cleared despite the disposal of the leather suite over 12 month ago. This patient tested positive to DMF and ethyl acrylate.
Patch test results are shown in Table 1.
Table 1: Positive patch test reactions in presented cases
The dermatitis affected the trunk, limbs, buttocks and even the face. The distribution of the dermatitis varied, and it later became apparent that this was due to the random distribution of the sachets containing DMF within the chairs and sofas. Many cases were suggestive of an acute irritant reaction or toxic erythema rather than an acute allergic contact dermatitis. Blistering and lichenoid eruptions were also observed. Few patients presented with contact urticaria.
Figure. 1 Weeping rash on back after sitting on a new recliner chair.

Many patients also complained of worsening of pre-existing asthma, wheezing and sneezing especially when on or around the chair or sofa. Patients complained of itching and stinging shortly after sitting on the chair or sofa. The dermatitis was often severe enough to require hospitalization. Symptoms started within 3 weeks to 9 months after purchasing a new chair, sofa or suite. Most patients recovered after disposing the furniture but sometimes after many months. In many patients, the symptoms would wax and wane before eventually settling.
This type of dermatitis was first discovered in Finland, although hundreds of cases have appeared in many other European countries. Hardly any patients suspected the furniture as the cause of their dermatitis. Most patients tested positive to the chair materials if the material was taken from the seat or the rest but not if the material was taken from the bottom of the chair. This led initially to suspect a finishing material sprayed on the furniture. Some patients tested positive to acrylates (e.g. ethyl acrylate, methyl acrylate) but the tests with commercial series did not show any consistent pattern. Fungicides were strongly suspected from the start as the cause of the dermatitis. The initial theory was that a chemical intended to be in a low concentration had accidentally been used at a much higher concentration.
Besides making dermatology more exciting, these types of dermatitis have outlined several important principles. Firstly, networking is a great asset in trying to solve an unusual or unexpected problem. Secondly, contact dermatitis induced by dimethylfumarate should be suspected in appropriate cases. However, it is also important to remember that this allergen is not included in most series for patch testing.
Adapted from J Eur Acad Dermatol Venereol 2010; 24: 486-9
















