Bronchonasal Crosstalk
The prevalence of asthma and rhinitis is increasing worldwide and environmental factors are mostly thought to be responsible for this. Both diseases frequently coexist in the same patients, with asthma present in 20-50% of patients with allergic rhinitis (AR) and rhinitis present in up to 80% of patients with asthma. The atopic status plays a potentially prominent role in this relationship, but this is not a prerequisite.
Epidemiologic evidence for the co-existence of upper and lower respiratory symptoms extends back more than 80 years. More revealing, however, are the many studies that have now shown that these conditions very frequently co-exist.
In 1920, Keller reported that among 100 case histories of patients with chest symptoms, 86 presented with concomitant nasal pathology. Keller hypothesized that "predominant mouth breathing secondary to persistent nasal congestion may have prevented the proper moistening, warming and filtering of the air, thus triggering asthma symptomatology." Since then, numerous studies have bolstered the epidemiologic link between asthma and the upper respiratory disorders.
Large longitudinal studies revealed that AR usually precedes the onset of asthma. Although such results have been interpreted to define AR as a risk factor for the development of asthma, rhinitis appears to be an early stage of combined allergic airways disease.
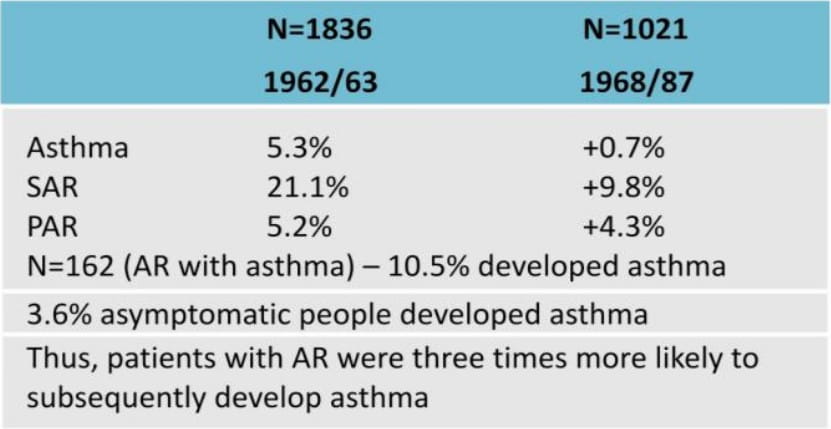
In a study carried out by Settipane et al, 690 individuals were resurveyed, 23 years after they had been originally surveyed when they were college freshmen in Rhode Island. These 690 individuals, now in their forties, were considered as a population at risk because, at the time of their first evaluation, they reported no diagnosis or symptoms compatible with asthma. However, 162 had a diagnosis of rhinitis. The incidence of asthma over the 23 years between the two surveys was 10.5% in the subjects with rhinitis and 3.6% in those without rhinitis ? a highly significant difference.
This indicates that individuals with AR are about three times more likely to develop asthma than negative controls.
Table 1: Result from the study carried out by Settipane et al, in patient with allergic rhinitis and asthma.
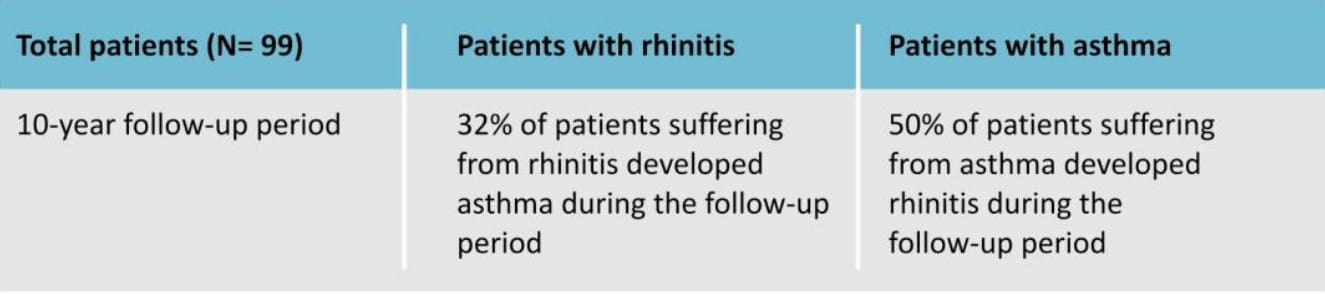
In a recent survey conducted at Genoa University, 99 patients were followed for up to 10 years after the initial diagnosis of AR, allergic asthma, or both. During the 10-year follow-up, the following observations were noted:
Table 2: Result of a survey conducted by Genoa University in patient with allergic rhinitis and asthma.
The Copenhagen Allergy Study reported that the frequency of allergic asthma among subjects with AR was 40-50%, whereas the frequency of allergic asthma among subjects without AR was 1 % or less. Consequently, the risk of asthma among subjects with AR was calculated to be up to 300 times that among subjects without AR.
Thus, going by this epidemiological data, there is a strong correlation between AR and asthma with AR preceding asthma in the majority of cases. The current concept is that AR precedes asthma in most patients, and when AR worsens, it negatively affects the course of asthma.
Therefore, published studies confirm the close epidemiologic association between AR and asthma. This has been acknowledged in several official position papers and international guidelines.
- AR and asthma can co-exist in the same patient.
- Asthma presents in 20-50% of patients with AR.
- Rhinitis presents in up to 80% of patients with asthma.
- AR precedes asthma.
- When AR worsens, it negatively affects the course of asthma.
Similarities and differences between the upper and lower airways
Figure 1: Anatomy of the respiratory tract.
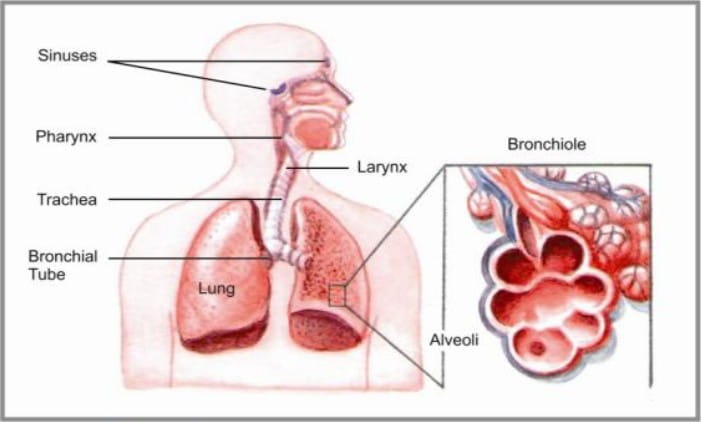
The respiratory tract can be considered as a single morpho-functional unit. It is entirely covered, up to the smaller bronchi, by ciliated epithelium and mucinous glands and an extensive vasculature and innervation (similar innervations in the upper and lower airways).
The respiratory mucosa is rich in mast cells, which are important effector and immunoregulatory units, and these cells are thought to significantly contribute to the nose-bronchi connection via cytokine release. Moreover, the lymphoid tissue constitutes the bronchial-(mucosal) associated lymphoid tissue (BALT or MALT), which is largely represented in both the nose and the bronchi.
Although these similarities exist between the nose and the lungs, cardinal differences also exist in that the nose and paranasal sinuses are rigid cavities, whereas the lower airways have an elastic parenchyma, rich in peribronchial smooth muscles.
This anatomical diversity accounts for the differential clinical features or symptoms to the same offending allergen such as sneezing, rhinorrhoea/blockage in the nose and bronchoconstriction in the lungs.
The upper respiratory tract acts as a filter, resonator, heat exchanger and humidifier for the inhaled air. The inhaled air is processed and enters into the bronchi with a temperature of about 37?C and almost completely saturated in humidity. The foreign particles greater than 5-6 p are efficiently removed and, therefore, filtered off from entering the lower airways. Thus, failure of any of these functions may result in an alteration of the homeostasis of the lower respiratory airways.
This anatomical correlation between the upper and lower respiratory tracts further strengthens the link between AR and asthma.
- The respiratory tract is a single morphofunctional unit.
- It is entirely covered by a ciliated epithelium and mucinous glands.
- Anatomical diversity accounts for the different clinical features to the same offending allergen.
It is now recognized that asthma and AR do not necessarily constitute distinct disease entities, but rather represent a final common pathway of closely related pathologic processes in the respiratory tract, with variable expression of severity and response to treatment. The onset of AR and asthma also appear to be temporally related, with upper airway symptoms often preceding or appearing at the same time as asthma.
In an allergic reaction, the early phase occurs within minutes. This early-phase reaction involves the release of histamine, vasodilatation, increased permeability, and bronchoconstriction.
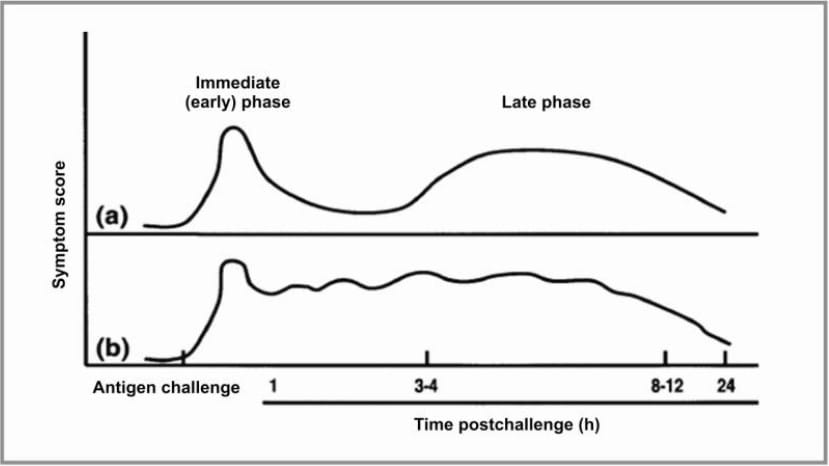
Figure 2 : Nasal symptoms after antigen challenge. More than 50% of patients with rhinitis may have a pattern similar to those depicted in the figure. A. After the acute reaction, symptoms dissipate and then recrudesce between 4 to 12 hours. B. Symptoms remain present for many hours after nasal challenge. (Adapted from Peebles R, Togias A, Late-phase reactions in the nose, in; Kay AB, editor. Allergy and allergic diseases, Oxford [UK]: Blackwell; 1997. p. 1139-60. With permission.)
This is followed by an inflammatory type of reaction called the late-phase allergic reaction in which T-lymphocytes, eosinophils, cytokines, chemokines and adhesion molecules play a part.
While the chemokines and cytokines act to induce the recruitment of cells into the target organ, the adhesion molecules are also crucial for the recruitment of these inflammatory cells by inducing the rolling over, extravasation and migration of cells from the blood vessels into the target organ.
These mechanisms have been seen in both AR and asthma, thus linking the upper and lower airways.
- Early AR occurs within the first few minutes.
- Early AR involves the release of histamine, vasodilatation, increased permeability and bronchoconstriction.
- Late AR takes 3-11 hours in which T-lymphocytes, eosinophils, cytokines, chemokines and adhesion molecules play a part.
- EAR & LAR is seen in both AR & Asthma
The clearest connection between AR and asthma is based on a shared physiological response; both are part of the body's immune response to an identified foreign substance.
When an allergen is presented, inflammatory cells and their progenitors immediately begin to proliferate in the bone marrow and move into the circulation. IgE molecules on the mast cells rapidly bind to the allergen, and after several IgE molecules are bound, the cross-linkages between them cause the mast cell to degranulate, releasing pre-formed mediators from the cell and initiating the production of other mediators in the inflammatory cascade.
The inflammatory response is similar for both AR and asthma as they share a similar respiratory epithelial structure of ciliated pseudostratified columnar epithelium with goblet cells. The pathophysiologies of local mediator release, systemic immune response and eosinophil recruitment are alike.
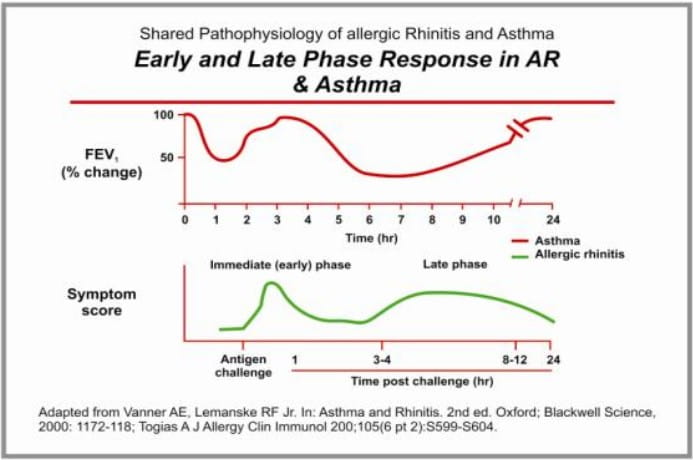
During the early-phase response, symptoms in patients with AR typically consist of sneezing, rhinorrhoea and conjunctivitis, while patients with asthma experience wheezing, coughing and shortness of breath, in addition to objectively demonstrable changes in lung function.
There is a similar pattern and time course of early- and late-phase responses in AR and asthma. Approximately 1 hour after allergen provocation, patients with AR experience a peak in symptoms, while patients with asthma experience a steep decline in lung function, measured by the forced expiratory volume in 1 sec (FEV1). During the late-phase response, nasal congestion is sustained in patients with AR, while a prolonged fall in lung function is again observed in patients with asthma. Within 12-24 hours, both types of reactions typically resolve.
Figure 3 : Early and late phase response in allergic rhinitis and asthma.
- On allergen exposure, the inflammatory cells proliferate in the bone marrow.
- Similar pattern and time course of early- and late-phase responses seen in AR and asthma.
- After allergen exposure, patients with AR experience a peak in symptoms, while patients with asthma experience a decline in lung function.
1. Bronchial Hyper-Responsiveness (BHR) in AR
One of the main clinical features of asthma is an increase in BHR. However, non-asthmatic subjects with AR can present BHR when exposed to an allergen to which they are sensitized. Studies have shown that nasal challenge can induce an increase in BHR.
A double-blind, placebo-controlled, crossover study explored the relationship between AR and lower airway dysfunction using randomized nasal challenges with either allergen or placebo in 11 subjects with a history of asthma exacerbations associated with seasonal symptoms of AR.
The technique used a nasal provocation that limited allergen (timothy grass extract) delivery only to the nose. After the induction of a marked nasal allergic response, no changes were observed in the FEV1 specific conductance, lung volumes or peak expiratory flow rates (PEFRs).
Yet, when compared with placebo, the allergen nasal provocation resulted in a significant increase in BHR to methacholine at 30 minutes and 4.5 hours after the challenge. These results demonstrate that although a nasal allergic response may not cause airflow limitation, it can enhance BHR in patients with asthma and AR.
The type and intensity of allergen exposure can play an important role in the clinical manifestations of atopy. Indoor allergens seem to be more frequently associated with BHR and asthma, while outdoor ones are more closely related to AR.
2. Nasal-Bronchial Reflex
In this paradigm, nasal stimulation promotes bronchoconstriction through a reflex arc, with the afferent arm located in the pharyngolaryngeal area, a central locus possibly in the hypothalamic area and vagal efferents.
The study that highlighted this theory included 6 patients without lung disease who underwent unilateral trigeminal nerve resection for trigeminal neuralgia. Upon insufflation of silica particles in the nares on the side where the trigeminal nerve was intact, a decrease in lung function and bronchoconstriction was effected whereas no bronchoconstriction was effected upon insufflation in the nares on the resected side. Bronchoconstriction in response to nasal silica was inhibited by previous topical atropine administration, suggesting that the bronchoconstriction could have resulted from activation of a cholinergic reflex arc.
3. Post-Nasal Drip of Inflammatory Material
Patients frequently complain that post-nasal drip triggers episodes of coughing and wheezing. Early studies investigating the possibility of aspiration of nasal secretion demonstrated that substances placed in the upper respiratory tract could later be recovered from the tracheobronchial tree.
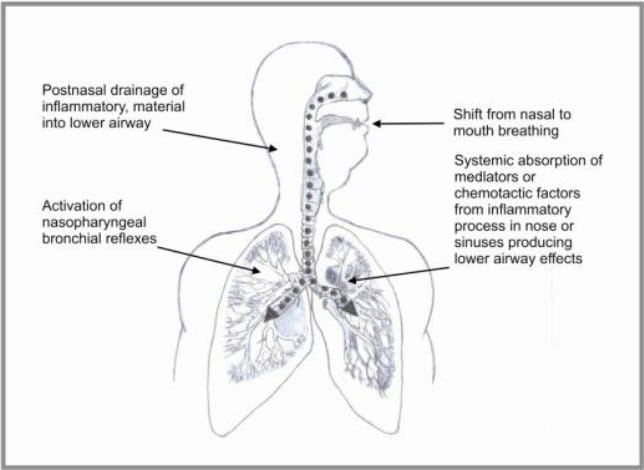
Figure 4 : Pathophysiological aspect for allergic rhinihs asthma link.
4. Immunological Evidence in the Linkages of Allergic Inflammation of the Upper and Lower Airways
AR and asthma are connected via an immunological response to airborne allergens that is evident throughout the entire body and through bronchial reaction to intranasal challenge. In keeping with the "united airways" concept, it has been shown that challenging the nose with relevant allergens may induce bronchial inflammation.
Braunstahl et al performed nasal allergen provocations in AR subjects without asthma and in normal control subjects. They observed an increase of eosinophils as well as increased expression of intercellular adhesion molecule-1 in nasal and bronchial biopsies of AR patients compared with controls.
In another study, Braunstahl and collaborators showed a decrease in the number of mast cells in the nose, interpreted as a result of degranulation, 24 hours after segmental broncho-provocation in non-asthmatic subjects with AR. Mast cells are considered key factors in the initiation of allergic inflammation, and this study further suggests that "crosstalk" between the upper and lower airways takes place at initiation of the inflammatory process, possibly through a systemic pathway, or via cytokine release of mast cells, which are abundantly present throughout the respiratory mucosa.
Link between the upeer and lower airways can be explained by the following:
- Bronchial hyper-responsiveness.
- Naso-bronchial reflex.
- Post-nasal drip of inflammatory cells.
- Immunological link.
The common co-morbidities and shared pathophysiologies of asthma and AR have led to the concept of "one airway, one disease" and the need for a common therapeutic approach. To achieve optimal treatment for patients, it is the recommendation of the Allergic Rhinitis and its Impact on Asthma (ARIA) workshop group in collaboration with the World Health Organization (WHO) that patients with persistent AR should be evaluated for asthma, and that patients with asthma should be evaluated for AR.
Two small studies in the 1980s showed benefits of intranasal corticosteroids for asthma symptoms. Effects of other treatments for co-morbid AR, including antihistamines, allergen immunotherapy, systemic anti- IgE therapy and anti-leukotriene agents, have been examined in a limited number of studies.
Recently published observational data also support the concept that asthma outcomes are better, for both children and adults, when co-morbid AR is treated. Crystal-Peters and coworkers evaluated data for almost 5,000 US patients aged 12-60 years with co-morbid AR and asthma. They found that, for the three-quarters of patients who were receiving treatment for AR, the risk of an asthma-related event (hospitalization or emergency department visits) was one-half that for patients not receiving treatment for AR.
Therefore, nasal therapy in AR patients with asthma has a beneficial effect on asthma symptoms, bronchial hyper-responsiveness and airway inflammation. Furthermore, it reduces the risk of asthma exacerbations. This stresses the importance of an integrated therapeutic approach involving both ends of the respiratory tract.
- All patients with persistent AR should be evaluated for asthma and patients with asthma should be evaluated for AR.
In summary, asthma and AR frequently occur concomitantly. The presence of AR often precedes the development of asthma and is a known risk factor for asthma. There is evidence that having co-morbid AR is a marker for the presence of more difficult-to-control asthma and, therefore, greater use of the resources for asthma. There are also strong indications from observational data that treating co-morbid AR may result in better asthma outcomes.
Important points to be noted are as follows:
- AR should be diagnosed properly in patients with asthma, as recommended in the Allergic Rhinitis and its Impact on Asthma Guidelines
- When AR is diagnosed, patients should be treated in the best possible way so as to avoid exacerbative episodes of asthma
At present, treatment typically follows a two-compartment model whereby asthma and AR are each treated separately and, often, locally or topically; treatment is administered seasonally for people with seasonal AR. Asthma outcomes might improve for patients with co-morbid AR and asthma if treatment was, instead, long-term and followed a combined therapeutic approach for the two conditions.
1. Indian Journal of Chest Diseases and Allied Sciences 2003; 45:179-189
2. Chinese Medical Journal 2006; 119:676-683
3. J Allergy Clin Immunol 1992; 89:611 -618
4. J Allergy Clin Immunol 2001; 107:469-476
5. Am J Respir Crit Care Med 2001; 164:858-865
6. Eur Respir Journal 1996; 9:905-909
7. J Allergy Clin Immunol 1992; 90:250-256
8. J Allergy Clin Immunol 1993; 91:97-101
9. J Allergy Clin Immunol 1997; 100:781 -788
10. J Allergy Clin Immunol 1995; 95:923-932
11. J Allergy Clin Immunol 2000; 105:917-922
12. J Allergy Clin Immunol 1998; 102:558-562
13. J Allergy Clin Immunol 2000; 6: S599-S604
14. Can Respir J Vol 2008; 15:91 -98
15. Southern Medical Journal 2009; 102:935-941
16. BMC Pulmonary Medicine 2006; 6:1 -7

















