

VERIFY: Early Initiation of Vildagliptin plus Metformin Delays Treatment Escalation in Treatment Naive Young-onset Diabetes Patients



Introduction
There is substantial prevalence of young-onset diabetes (YOD; onset before the age of 40 years). Longer disease duration and suboptimal control of cardiometabolic risk factors hike the risk of premature complications and mortality in patients with YOD. In absence of long-term efficacy and safety data of pharmacological interventions, treatment initiation and intensification is often delayed in patients with YOD.
Aim
To determine the glycaemic durability (sustained glycaemic control) with early combination therapy (metformin plus vildagliptin) vs. initial metformin monotherapy, among patients with type-2 diabetes mellitus (T2DM) with YOD and late-onset diabetes (LOD; the onset age of 40 years)
Patient Profile
- Participants form the VERIFY (The Vildagliptin Efficacy in combination with metfoRmIn For earlY treatment of type 2 diabetes) trial.
- All subjects had glycated haemoglobin (HbA1c) level of 6.5–7.5% and body-mass index (BMI) of 22–40 kg/m² (n=2001)
- Patients were stratified based on their age as follows:
- Young onset diabetes (YOD): Age of onset >40 years
- Late onset diabetes (LOD): Age of inset <40 years
Methods
Study Design
- A substudy of VERIFY trial
- VERIFY was a randomized, double-blind, multinational, multi-ethnic, two-arm parallel-group study
Treatment Strategy
- Following a three-week run-in phase of metformin treatment, patients were randomized 1: 1 as follows:
- Early combination group: Vildagliptin (50 mg twice-daily) added to metformin
- Monotherapy group: Placebo (Period 1) followed by the addition of vildagliptin (50 mg twice-daily) only after a confirmed initial treatment failure (TF; earliest at six months, transferring the patients to Period 2)
- All patients received vildagliptin plus metformin during period 2, irrespective of their initial trial.
- After the secondary TF during period 2 (12-month visit; transferring patient to Period 3), open-label insulin could be initiated as an add-on to the combination therapy.
Outcomes
- Time to initial TF, defined as HbA1c ≥7.0% at two consecutive scheduled visits after randomization
- Rates of primary and secondary TF
- Changes in body-weight and urinary albumin/creatinine ratio
- Treatment-emergent adverse events (AEs) and serious AEs (SAEs)
Results
- Of the entire study population, 186 (9.3%) patients had YOD and 1815 (90.7%) had LOD. The mean age difference between YOD and LOD groups was 20.4 years.
- Compared with initial metformin monotherapy, early combination therapy reduced the risk of initial TF by 48% in patients with YOD and by 46% in patients with LOD (Fig. 1).
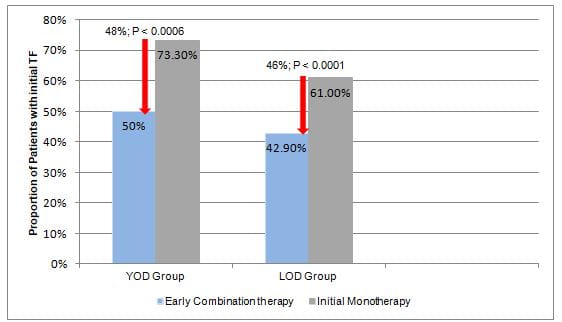
- The median time to TF was longer with combination therapy vs. monotherapy in both, YOD and LOD groups. The reduction in risk to initial TF with early combination vs. monotherapy did not differ significantly between patients with YOD and LOD (Table. 1).
|
|
Early Combination Group |
Initial Monotherapy Group |
HR (95% CI) |
Risk reduction |
P value |
|
Patients with YOD |
41.9 months |
26.9 months |
0.52 (0.36–0.76) |
48% |
0.0006 |
|
Patients with LOD |
61.9 months |
38.6 months |
0.54 (0.48–0.62) |
46% |
<0.0001 |
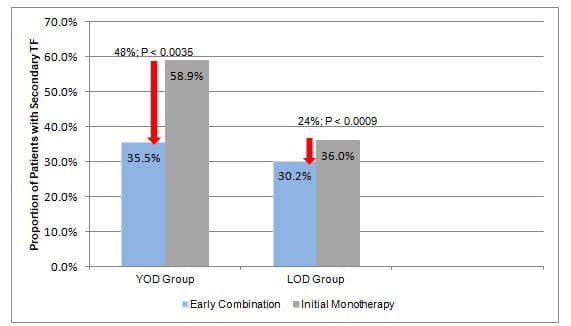
- Early combination reduced the risk of secondary TF by 48% in patients with YOD and by 24% in patients with LOD (Fig 2).
- Urinary albumin/creatinine ratio and body-weight remained stable with both treatment approaches in patients with YOD and LOD.
- The safety and tolerability profile was similar for both the treatment approaches. Both treatment approaches were well tolerated with no unexpected safety concerns.
Conclusion
- Initiating early combination strategy (vildagliptin plus metformin) in treatment-na?ve patients with YOD (HbA1c; 6.5−7.5%) improved attainment of the glycaemic target and durability; and delayed treatment escalation compared with sequential treatment of metformin followed by addition of vildagliptin.
Diabetes Obes Metab. 2020 Sep, 7 (Published Online); doi: 10.1111/dom.14192.












