

TRANSITION Study: Feasible and Safe to Initiate Sacubitril/Valsartan Pre-discharge in Acute HFrEF



Background
Hospitalizations due to decompensated heart failure (HF) increase the burden of mortality and re-hospitalization in HF patients. This risk is high especially during the initial 2-3 months, when mortality can reach up to 10% in these patients. Hospitalizations thus provide a crucial opportunity to initiate and up-titrate the guideline-recommended therapies to improve post-discharge prognosis. The PARADIGM-HF trial has already demonstrated the superiority of sacubitril/ valsartan over enalapril for reducing mortality and morbidity in ambulatory patients with chronic heart failure with reduced ejection fraction (HFrEF)
Aim
The TRANSITION study aimed to provide the real-world data on safety and tolerability of initiating sacubitril/valsartan in HFrEF patients following hemodynamic stabilization after acute decompensated HF (ADHF) requiring hospitalization.
Patient Profile
- Patients with HFrEF, New York Heart Association (NYHA) class II−IV, left-ventricular ejection fraction (LVEF) ≤40% following hemodynamic stabilization* after an episode of ADHF.
- Patients were stratified based on their pre-treatment status as follows:
o Receiving an angiotensin-converting enzyme inhibitor (ACEI)
o Receiving an angiotensin receptor blocker (ARB)
o ACEI/ARB-na?ve patients
*Hemodynamic stabilization defined as no need for intravenous diuretics in 24 h prior to screening and systolic blood pressure [SBP] >110 mm Hg for at least 6 h prior to randomization
Methods
Study Design
- A randomized, parallel, open-label study comparing pre- versus post-discharge (1–14 days) initiation of sacubitril/valsartan in the study population
Treatment Strategy
- Patients were randomized 1:1 within each stratum for initiation of sacubitril/valsartan treatment either pre- or post-discharge (Figure 1)
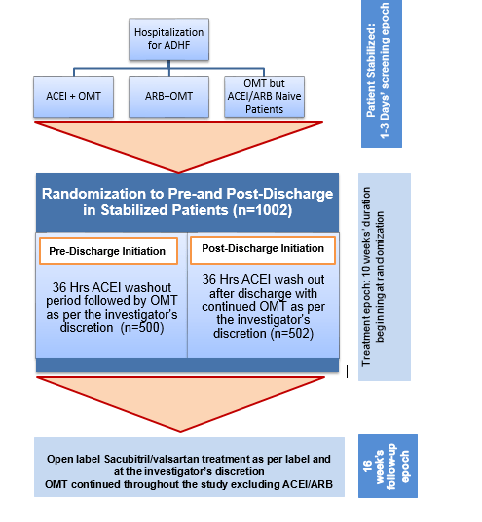
OMT: Optimized medical treatment
Endpoints
Primary Endpoint
- The proportion of patients achieving the target dose of 200 mg sacubitril/valsartan twice daily, at 10 weeks’ post-randomization
Secondary Endpoints
- The tolerability of different doses of sacubitril/valsartan (200 mg, 100 mg, or any other dose) maintained for a period of 2 weeks or more, leading to week 10 after randomization
- The incidence of permanent discontinuation of sacubitril/valsartan due to adverse events (AEs)
Results
- Mean age of the study population at baseline was 67 years and 75% of them were male. Mean LVEF for the study population was 29%, 64% belonged to NYHA Class II and 34% to NYHA III.
- There were 286 (29%) cases of new-onset HFrEF and 242 (24%) patients were ACEI/ARB na?ve.
- Similar proportion of patients met the primary and secondary endpoints in the pre- and post-discharge initiation arms
- At 10 weeks after randomization, there was statistically no significant difference in proportion of patients who achieved the target dosage of 200 mg twice daily between the pre-discharge and the post-discharge arm (45% vs. 50.4%; 95% CI 0.783–1.019; p=0.092) (Figure 2).
- Nearly two-thirds of patients initiated on sacubitril/valsartan pre-discharge and post-discharge , achieved and maintained either 100 mg or 200 mg twice daily regimen for at least 2 weeks following 10 weeks of randomization (62.5% and 68%, respectively; p=0.071) (Figure 2)
- Majority of patients in pre-discharge and post-discharge arm (86.4% vs. 88.8%,, p=0.262) achieved and maintained any dose of sacubitril/valsartan for at least 2 weeks following 10 weeks of randomization (Figure 2)
- The rate of permanent discontinuation of study drug due to adverse events (AEs) was low amongst patients in both, the pre-discharge and post-discharge arms (4.5% vs. 3.5%, RRR; 1.287, p=0.424)
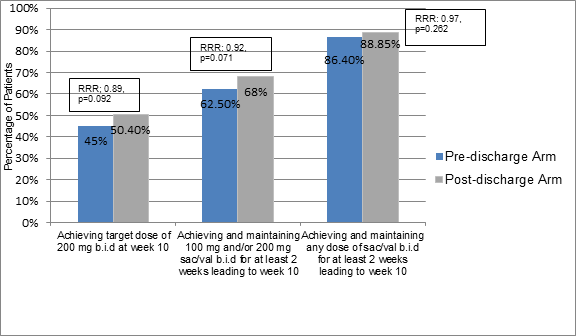
Sac/val: sacubitril/valsartan, b.i.d: twice daily
- Hyperkalemia, hypotension, cardiac failure, and dizziness were the most frequently reported AEs in both the study arms and had almost a similar incidence between the two groups. (Table 1)
|
Adverse Event |
Pre-discharge Group |
Post-discharge Group |
|
Hyperkalemia |
11.1% |
11.3% |
|
Hypotension |
12.3% |
9.1% |
|
Cardiac Failure |
6.8% |
8.5% |
|
Dizziness |
5.6% |
4.2% |
- Nearly 18.9% patients in the pre-discharge arm and 17.7% in the post-discharge arm suffered with serious AEs (SAEs). Of these, cardiac failure was the most common (7.0% vs. 7.7% of patients in the pre- vs. post-discharge group, respectively)
- Patients in both the treatment arms had low mortality (2.6% vs. 2.0% in pre- vs. post-discharge arm; p=0.6740). None of the deaths were attributed to the study treatment
Conclusion
- Nearly 50% of the HFrEF patients who were hemodynamically stabilized following an ADHF event attained the recommended target dose of 200 mg sacubitril/valsartan twice daily within 10 weeks
- Patients in the pre-and post-discharge arms had similar incidence of AEs. The rate of discontinuation of sacubitril/valsartan due to adverse events was also similar in both the study arms.
- The patient subgroups that tolerated the up-titration of sacubitril/valsartan to target dose within 10 weeks included; those with fewer comorbidities, higher systolic blood pressure or newly diagnosed HF.
- Sacubitril/valsartan was safe and effective in patients stabilized after hospitalization for acute HF regardless of whether they received it in-hospital or after discharge.
Presented at the European Society of Cardiology (ESC) Congress-2018, Aug 25-29, 2018; Munich, Germany
|
|











