

TRANSITION: Impact of Sacubitril/valsartan on NT-proBNP in Hospitalized HFrEF Patients



Introduction
N-terminal pro-B type natriuretic peptide (NT-proBNP) is a marker of cardiac wall stress and a predictor of event risk in patients with acute decompensated heart failure (ADHF). Several trials till date have demonstrated that sacubitril/valsartan treatment was associated with reduction in NT-proBNP and a subsequent improvement in cardiac remodelling and function in patients with HF with reduced ejection fraction (HFrEF), including those hospitalized for ADHF.
Aim
To determine the impact of sacubitril/valsartan on NT-proBNP levels and to ascertain patient characteristics associated with favourable NT-proBNP reduction response.
Patient Profile
- Patients hospitalized for an episode of ADHF (age ≥18 years; n=991)
- All patients had a reduced ejection fraction [left ventricular ejection fraction (LVEF) ≤40%) and New York Heart Association (NYHA) class II to IV. Blood pressure at screening was ≥100 mmHg
Methods
Study Design
- TRANSITION (Comparison of Pre- and Post-discharge Initiation of Sacubitril/Valsartan Therapy in HFrEF Patients After an Acute Decompensation Event) was a randomized, multi-centre, open-label study conducted in 156 hospitals across 19 countries
- The current study was a post-hoc analysis of TRANSITION study
Treatment Strategy
- Patients were randomized 1:1 to open-label sacubitril/valsartan initiation either in-hospital (pre-discharge) or post-discharge as follows:
- Pre-discharge group: First dose of sacubitril/valsartan no later than 12 h before discharge and ≤7 days after randomization (n=495)
- Post-discharge group: First dose of sacubitril/valsartan at any time between days 1 and 14 post-discharge (n=496)
- Sacubitril/valsartan was up-titrated to achieve and maintain a dose of 97/103 mg twice daily along with optimized therapy for HFrEF.
Assessments
- NT-proBNP was measured at randomization (baseline), at discharge, and at week 4 and 10, post-randomization.
Outcomes
- A favourable NT-proBNP response, defined as; reduction to ≤1,000 pg/ml or >30% from baseline
Results
- The median NT-proBNP levels at baseline did not differ significantly between patients in pre-discharge group (1902 pg/ml) and post-discharge group (1669 pg/ml).
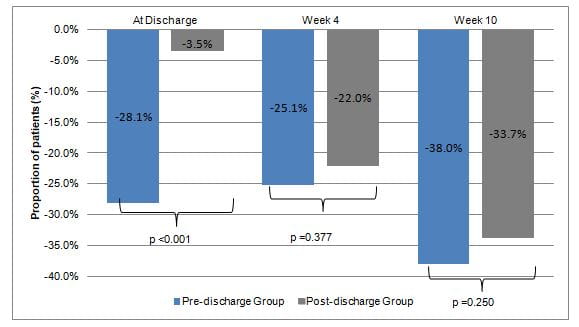
- At discharge, patients in the pre-discharge group had a greater decrease in NT-proBNP levels when compared to the patients in the post-discharge group (28%; p<0.0001 vs. 4%; p=0.293; between group difference p<0.001). Reduction in NT-proBNP was similar in both groups at week 4 (and week 10, post-randomization (Figure 1).
- Similarly greater proportion of patients in pre-discharge group vs. post-discharge group achieved favourable NT-proBNP response at discharge, though similar proportion of patients in both the groups achieved favourable response to NT-proBNP at week 4 and 10 (Table 1)
|
Time point during the study |
Pre-discharge Group |
Post-discharge Group |
|
At discharge |
46.2% |
18.2%% |
|
Week 4 |
46.2% |
41.6% |
|
Week 10 |
51.2% |
48.2% |
- Patients with a favourable NT-proBNP response at week 4 had a 43% lower risk of first HF rehospitalization or cardiovascular death through 26 weeks [hazard ratio (HR); 0.57; 95% confidence interval (CI): 0.38 to 0.86; p = 0.007).
- Predictors of a favourable response at week 4 and week 10 were similar and included; higher initial dose of sacubitril/valsartan (≥49/51 mg twice daily), higher baseline NT-proBNP, lower baseline serum creatinine, de novo HF, no atrial fibrillation, angiotensin-converting enzyme inhibitor–naive or angiotensin receptor blocker–naive, no mineralocorticoid receptor antagonist at baseline, no prior myocardial infarction, and higher weight.
Conclusions
- In-hospital initiation of sacubitril/valsartan in patients with ADHF was associated with rapid and significant reductions in NT-proBNP at discharge.
- Favourable NT-proBNP response over time; as predicted by higher starting dose and predisposing clinical profile was associated with a better prognosis.
- The findings of this study support the strategy of early in-hospital initiation of sacubitril/valsartan in patients hospitalized with ADHF.
JACC Heart Fail. Aug 7, 2020 (Published Ahead of Print); doi: 10.1016/j.jchf.2020.05.012.












