

High-dose atorvastatin therapy yields incremental benefits in patients with CHD and metabolic syndrome, irrespective of the presence of diabetes: Sub-analysis of Treating to New Targets (TNT) study
TNT: Sub-analysis in CHD Patients with Metabolic Syndrome

28 Oct, 10


TNT: Sub-analysis in CHD Patients with Metabolic Syndrome
Introduction
Background
- Metabolic syndrome is a clustering of cardiovascular risk factors including insulin resistance, obesity, hypertension, and dyslipidaemia, and is closely linked to the development of diabetes and cardiovascular disease.
- There is a paucity of data on the effects of statins on cardiovascular morbidity and mortality in patients with the metabolic syndrome
Objective
To evaluate whether intensive lipid-lowering with high-dose atorvastatin provides significant clinical benefit as compared to standard atorvastatin therapy in patients with coronary heart disease (CHD) and metabolic syndrome
Study Design and Participants
Post hoc analysis of TNT study participants (5584 patients with metabolic syndrome and CHD and having LDL <130 mg/dl)
Interventions
Atorvastatin 10 mg/day (n= 2820) or atorvastatin 80 mg/day (n=2764)
Follow-up
Mean of 4.9 years
Outcome Measures
- Primary efficacy outcome was the time to first occurrence of a major cardiovascular event [CHD death, nonfatal non-procedure-related myocardial infarction (MI), resuscitated cardiac arrest, and fatal or nonfatal stroke]
- Secondary efficacy outcome included any cardiovascular event, major coronary event (CHD death, nonfatal non-procedure-related MI, or resuscitated cardiac arrest), any coronary event, cerebrovascular event, peripheral arterial disease, documented angina, hospitalization for congestive heart failure, and all-cause mortality
Results
A) Effect on Lipids
After 3 months of treatment, the levels of LDL and triglycerides were significantly lower with atorvastatin 80 mg as compared to atorvastatin 10 mg (Figure 1)
Figure 1. Changes in lipids
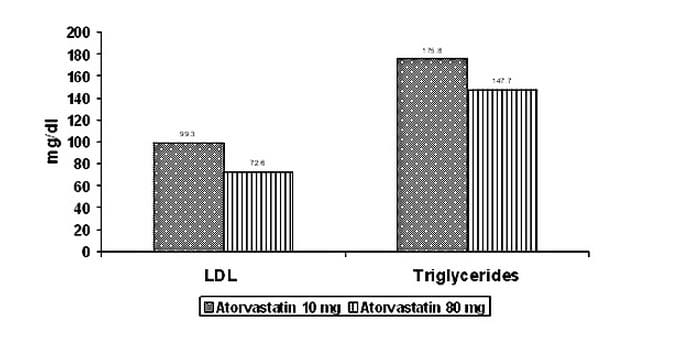
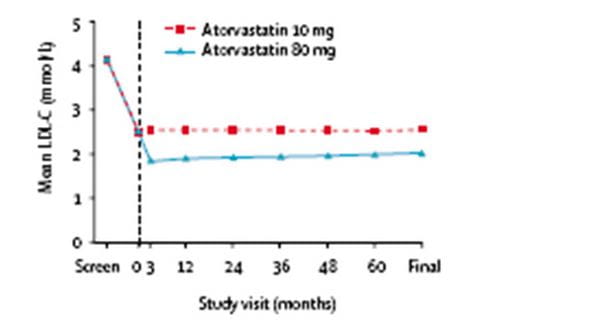
Figure 2 summarizes changes in LDL during the study in the two groups
Figure 2. Mean LDL levels during the study in both groups
B) Effect on Primary and Secondary Outcomes
In patients with metabolic syndrome and CHD
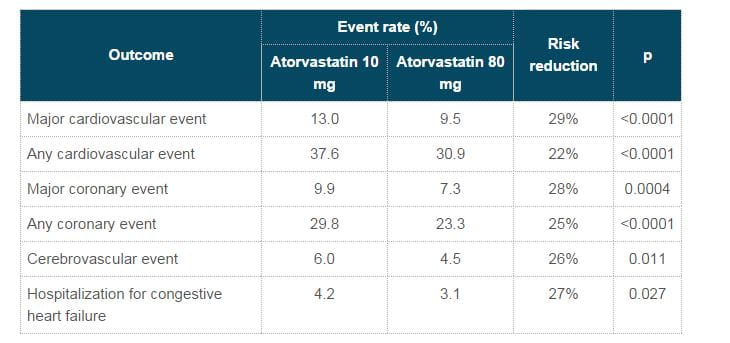
Atorvastatin 80 mg showed significant reduction in outcomes vs. atorvastatin 10 mg (Table 1)
Table 1: Comparison of event rates with atorvastatin 80 mg vs. 10 mg
In patients with metabolic syndrome and CHD without diabetes at screening
- Atorvastatin 80 mg significantly reduced the risk of major cardiovascular event by 30%
- For most secondary outcomes, the beneficial effect with atorvastatin 80 mg were similar to those observed in all patients with metabolic syndrome and CHD
Incremental increase in cardiovascular risk attenuated with atorvastatin 80 mg
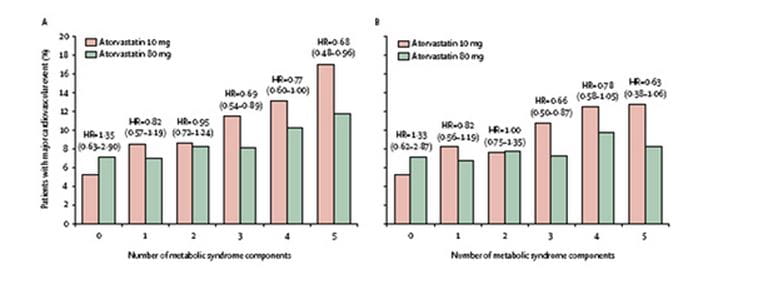
- An incremental increase in the risk of cardiovascular events with each additional component of the metabolic syndrome was attenuated only with atorvastatin 80 mg (Figure 2A).
- Similar results were seen in all patients without diabetes (Figure 2B).
Figure 2 A/B. No. of patients with major cardiovascular events by presence of metabolic syndrome components in (A) all TNT patients (n=10001), and (B) all TNT patients without diabetes (n=8500)
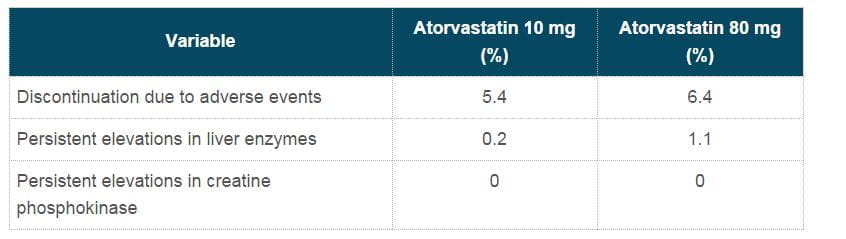
C) Safety
The prevalence of adverse events related to treatment were similar in both groups
Table 2. Comparison of adverse effects
Clinical Implications
- A total of 28 patients with metabolic syndrome and CHD without diabetes would needed to be treated for 5 years with atorvastatin 80 mg to prevent 1 major cardiovascular event
- A total of 29 patients with metabolic syndrome and/or diabetes with CHD would needed to be treated for 5 years with atorvastatin 80 mg to prevent 1 major cardiovascular event
Conclusion
- A greater LDL lowering than that achieved with standard doses of statins is warranted in patients with CHD and metabolic syndrome
"The two post-hoc analyses of TNT in patients with diabetes and/or metabolic syndrome support the concept of the higher the risk, the greater the need to treat and to treat aggressively."
A. J. Scheen, Dept. of Medicine, Belgium, in an editorial comment.
Lancet 2006;368:919-28

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


