

Tigecycline Monotherapy vs. Imipenem/Cilastatin in Hospitalized Chinese Patients with cIAIs



Background
The management of complicated intra-abdominal infections (cIAIs) remains a challenge to physicians because of their polymicrobial nature coupled with the high risk of sequelae and mortality in severely ill patients with these infections. Tigecycline, a first-in-class expanded broad-spectrum glycylcycline antibiotic approved for use in patients with cIAIs, overcomes the 2 major mechanisms of resistance to tetracycline.
Aim
To evaluate safety and efficacy of tigecycline monotherapy vs. imipenem/cilastatin in hospitalized Chinese patients with cIAIs
Patients Profile
- Men and non-pregnant, non-lactating women ≥18 years of age who required a surgical procedure for a complicated intra-abdominal infection (cIAI)
- cIAI defined as the following:
- An intra-abdominal abscess (including liver and spleen) that developed in a postsurgical patient after receiving standard antibacterial therapy (i.e., at least 48 hours, but not more than 5 days of antibiotics)
- Appendicitis complicated by perforation and/or a periappendiceal abscess
- Perforated diverticulitis complicated by abscess formation or fecal contamination
- Complicated cholecystitis with evidence of perforation or empyema
- perforation of a gastric or duodenal ulcer with symptoms exceeding 24 hours
- Purulent peritonitis or peritonitis associated with fecal contamination
- Perforation of the large or small intestine with abscess or fecal contamination, or traumatic bowel perforation with symptoms lasting at least 12 hours before an operation
Methods
Study Design
- Phase 3
- Multicenter
- Open-label study
- Patients (N=199) were randomly (1:1) assigned to receive IV tigecycline (n=97) or imipenem/cilastatin (n=102) for ≤2 weeks
Interventions
- Tigecycline: initial 100-mg dose given by intravenous [IV] infusion
over a 30-minute period, followed by 50 mg IV every 12 hours
- IV imipenem/cilastatin: :500 mg/500 mg every 6 hours or dose-adjusted based on weight and creatinine clearance
Study Endpoints
- Clinical response at the test-of-cure visit (12-37 days after therapy) for the microbiologic modified intent-to-treat (m-mITT) and microbiologically evaluable (ME) populations
- Microbiological response at the TOC visit by patient and isolate was performed as a secondary analysis
Results
Clinical Efficacy
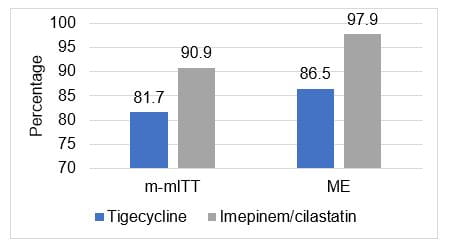
- Tigecycline-treated patients with polymicrobial infection tended to have lower clinical cure rates compared with patients who had monomicrobial infection
|
|
|
Tigecycline |
Imipenem/ cilastatin |
Difference (Tigecycline-Imipenem /cilastatin) |
| |
|
Population |
N |
% |
N |
% |
|
|
|
ME |
45/52 |
86.5 |
47/48 |
97.9 |
-11.4 |
|
|
Monomicrobial |
30/33 |
90.9 |
25/26 |
96.2 |
-5.2 |
|
|
Polymicrobial |
15/19 |
78.9 |
22/22 |
100.0 |
-21.1 |
|
|
m-mITT |
49/60 |
81.7 |
50/55 |
90.9 |
-9.2 |
|
|
Monomicrobial |
32/38 |
84.2 |
27/29 |
93.1 |
-8.9 |
|
|
Polymicrobial |
17/22 |
77.3 |
23/26 |
88.5 |
-11.2 |
|
|
Clinically Evaluable |
67/77 |
87.0 |
83/87 |
95.4 |
-8.4 |
|
|
Clinical – mITT |
78/97 |
80.4 |
88/98 |
89.8 |
-9.4 |
|
- Tigecycline was effective across the range of clinical diagnoses.
- Clinical cure rates at the TOC visit for the ME population were 87.0% for tigecycline and 100.0% for imipenem/cilastatin
|
|
|
Tigecycline |
Imipenem/cilastatin |
Difference (Tigecycline-Imipenem/cilastatin) | |
|
Diagnosis |
N |
|
N |
% |
% |
|
Complicated appendicitis |
40/46 |
87.0 |
45/45 |
100 |
-13.0 |
|
Complicated cholecystitis |
2/2 |
100.0 |
0/0 |
NA |
NA |
|
Peritonitis |
2/3 |
66.7 |
2/3 |
66.7 |
0.0 |
|
Gastric/duodenal perforation |
1/1 |
100.0 |
0/0 |
NA |
NA |
Microbial Efficacy
- In the ME population, the baseline organisms were eradicated in 86.5% of tigecycline-treated patients and 97.9% of patients treated with imipenem/cilastatin at the TOC visit
- For E. coli, the most commonly isolated bacteria, eradication rates were 88.1% for tigecycline vs. 97.7% for imipenem/ cilastatin
- Overall, MIC values for tigecycline against the most commonly isolated aerobes and anaerobes was ≤2.0 ?g/mL
- For E.coli , MIC50 and MIC90 values were 0.125 ?g/mL and 0.5 ?g/mL for tigecycline, respectively, and 0.25 ?g/mL and 0.5 ?g/mL for imipenem/cilastatin, respectively
Safety
- Tigecycline monotherapy was generally well tolerated in this study population
- The overall incidence of treatment-emergent AEs was significantly higher after tigecycline therapy (80.4%) compared with imipenem/cilastatin (53.9%; P < 0.001).
- gastrointestinal-related events, especially nausea (21.6% vs. 3.9%; P < 0.001) and vomiting (12.4% vs. 2.0%; P = 0.005)
Conclusions
- Tigecycline monotherapy appears to be both effective and safe for the treatment of cIAI in Chinese patients
- Clinical cure rates and safety profile for tigecycline were consistent with those found in global cIAI studies
- Digestive-related adverse events were significantly higher in the tigecycline group, especially nausea and vomiting
Reference
BMC Infectious Diseases 2010 10:217.












