

TANGO I Trial: Meropenem-Vaborbactam vs Piperacillin-Tazobactam for Treatment of Complicated Urinary Tract Infection



Introduction
Carbapenem-resistant Enterobacteriaceae infections are most often urinary tract infections (UTIs), including acute pyelonephritis, and are usually health care– associated. Mortality due to these infections is 20% to 54.3% and reflects the need for better treatment options. Vaborbactam plus meropenem was developed as a fixed combination product for severe gram-negative infections, including those due to carbapenem-resistant Enterobacteriaceae. It has potent in vitro activity against K pneumoniae carbapenemase-producing carbapenem-resistant Enterobacteriaceae and restores activity of meropenem in animal models of infections due to these organisms.
Aim
Targeting Antibiotic Non-Susceptible Gram-Negative Organisms (TANGO I) randomized clinical trial was conducted to evaluate efficacy and adverse events of meropenem-vaborbactam in complicated urinary tract infection (UTI), including acute pyelonephritis.
Patient profile
- N=550
- Patients (≥18 years) with complicated UTI, stratified by infection type and
- geographic region.
- 185 kg or less
- needed 5 or more days of intravenous antibiotics
- documented or suspected complicated UTI or acute pyelonephritis
|
Baseline Characteristics (MITT Population) a |
No. (%) Meropenem- Vaborbactam (n = 272) |
Piperacillin- Tazobactam (n= 273) |
|
Acute pyelonephritis |
161 (59.2) |
161 (59.0) |
|
Complicated urinary tract infection |
111 (40.8) |
112 (41.0) |
|
With removable source of infection b |
53 (19.5) |
51 (18.7) |
|
With nonremovable source of infection |
58 (21.3) |
61 (22.3) |
|
Age, mean (SD), y |
53.0 (19.4) |
52.6 (20.9) |
|
≥65 |
87 (32.0) |
103 (37.7) |
|
Female sex |
181 (66.5) |
180 (65.9) |
|
White race |
254 (93.4) |
252 (92.3) |
|
Creatinine clearance, mean (SD), mL/min/1.73 m2 |
93.5 (34.4) |
89.2 (36.4) |
|
≤50 |
31 (11.4) |
37 (13.5) |
|
Diabetes mellitus |
42 (15.4) |
44 (16.1) |
|
Systemic inflammatory response syndromec |
77 (28.3) |
90 (33.0) |
|
Charlson Comorbidity Index score ≥3d |
143 (52.6) |
147 (53.8) |
|
Common baseline pathogens (microbiologic MITT population) e,f |
n = 192 |
n = 182 |
|
Escherichia coli |
125 (65.1) |
117 (64.3) |
|
Klebsiella pneumoniae |
30 (15.6) |
28 (15.4) |
|
Enterococcus faecalis |
13 (6.8) |
14 (7.7) |
|
Proteus mirabilis |
6 (3.1) |
12 (6.6) |
|
Enterobacter cloacae species complex |
10 (5.2) |
5 (2.7) |
|
Drug resistance (FDA/CLSI criteria) in the most common baseline urinary gram-negative pathogens (microbiologic MITT population) a,g,h |
|
|
|
E coli |
n = 124 |
n = 115 |
|
Meropenem |
0 |
0 |
|
Piperacillin-tazobactam |
7 (5.6) |
6 (5.2) |
|
K pneumoniae |
n = 30 |
n = 27 |
|
Meropenem |
1 (3.3) |
2 (7.4) |
|
Piperacillin-tazobactam |
15 (50) |
9 (33.3) |
Abbreviations: CLSI, Clinical and Laboratory Standards Institute; FDA, US Food and Drug Administration; MITT, modified intent-to-treat.
aPopulation comprised all patients who received 1 or more doses of study drug.
bIncludes urinary catheter or removable kidney stones.
cDefined as the occurrence of ≥2 of fever (temperature >38°C [100.4°F]) or temperature <36°C (96.8°F); heart rate >90/min; respiratory rate >20/min or arterial carbon dioxide tension <32 mm Hg; abnormal white blood cell count (>12 000/μL or <4000/μL or >10% immature [band] forms).
dIndex used to categorize comorbidities based on ICD diagnosis codes. Each category has an associated weight (range, 1-6), based on adjusted risk of mortality or resource use. The sum of weights results in a comorbidity score; higher score indicates higher likelihood that the predicted outcome will result in mortality or higher resource use.
eOrganisms observed in ≥15 patients at baseline. Some patients had >1 pathogen at baseline. Overall, in the microbiologic MITT population, 12 of 192 patients (6.3%) in the meropenem-vaborbactam group and 20 of 182 (11.0%) in the piperacillin-tazobactam group had >1 baseline pathogen.
fThe microbiologic MITT population included all patients in the MITT population with bacterial pathogens of ≥10
CFU/mL in baseline urine culture or the same bacterial pathogen present in concurrent blood and urine cultures.
gThe FDA/CLSI breakpoint for piperacillin-tazobactam resistance of Enterobacteriaceae is >64 μg/mL. The FDA/CLSI breakpoint for meropenem resistance of Enterobacteriaceae is ≥4 μg/mL.
hOnly pathogens with a frequency of at least 10 patients total are included. Only data from urinary isolates are included. If the same pathogen was isolated from the same source (urine or blood), only the result for the isolate with the highest minimum inhibitory concentration was included
Methods
- TANGO 1 is a Phase 3, multicenter, multinational, randomized clinical trial
- November 2014 to April 2016
- 60 sites in 17 countries
- 550 patients were randomized 1:1 to receive
- meropenem-vaborbactam (2g/2g over 3 hours; n = 274) every 8 hours
- piperacillin-tazobactam (4g/0.5g over 30 minutes; n = 276) every 8 hours
Primary Endpoint
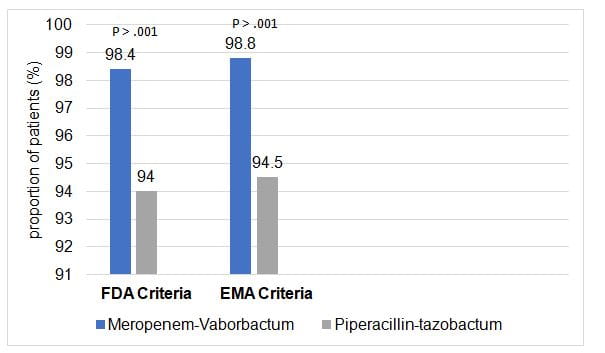
- For FDA criteria was overall success (clinical cure or improvement and microbial eradication composite) at end of intravenous treatment in the microbiologic modified intent-to-treat (ITT) population
- For European Medicines Agency (EMA) criteria was microbial eradication at test-of-cure visit in the microbiologic modified ITT and microbiologic evaluable populations
Secondary Endpoint
- Proportion of patients with overall success at end of intravenous treatment and at test-of-cure visits (by infection type) in the microbiologic modified ITT population
- Clinical cure at end of intravenous treatment and at test-of-cure visits in the microbiologic modified ITT population
- Microbial eradication to less than 10 CFU/mL of urine for the FDA criteria and less than 10 CFU/mL of urine for the EMA criteria at end of intravenous treatment and at test-of-cure visits in the microbiologic modified ITT and microbiologic evaluable populations per-pathogen outcomes (overall success, clinical cure, and microbial eradication) in the microbiologic modified ITT population
- Adverse event and tolerability profile of meropenem-vaborbactam as assessed by vital signs clinical laboratory tests electrocardiograms physical examinations
Results
Primary Endpoint
- At end of intravenous treatment, noninferiority was met for the FDA primary end point of overall success in the microbiologic modified ITT population and for the EMA primary end point of microbiologic outcome of eradication at test of cure in the microbiologic modified ITT and microbiologic evaluable populations
|
Key secondary Endpoints |
Meropenem-vaborbactam |
Piperacillin-tazobactam |
|
Overall success at test to cure |
74.5 |
70.3 |
|
Overall success at the end of intravenous treatment |
|
|
|
acute pyelonephritis |
97.5 |
94.3 |
|
complicated UTI, removable source of infection |
100 |
92.1 |
|
Complicated UTI, nonremovable source of infection |
100 |
95.3 |
|
Clinical cure at end of intravenous treatment |
98.4 |
95.6 |
|
Clinical cure at test at cure |
90.6 |
86.3 |
|
Microbial Eradication |
97.9 |
92.3 |
|
Microbial eradication at test of cure |
68.8 |
62.1 |
Adverse Events
Meropenem-vaborbactam was well tolerated 2.6% of patients discontinuing study treatment discontinuation due to adverse event compared with 5.1% discontinuing piperacillin-tazobactam
- Overall incidence of adverse events and serious adverse events was numerically similar between treatment groups
- Adverse events were reported
- 106 of 272 (39.0%) with meropenem-vaborbactam
- 97 of 273 (35.5%) with piperacillin-tazobactam
|
Adverse Event |
No. (%)b |
|
|
|
Meropenem-Vaborbactam (n= 272) |
Piperacillin-Tazobactam (n =273) |
Total (n =545) |
|
|
Headache |
24 (8.8) |
12 (4.4) |
36 (6.6) |
|
Diarrhea |
9 (3.3) |
12 (4.4) |
21 (3.9) |
|
Nausea |
5 (1.8) |
4 (1.5) |
9 (1.7) |
|
Asymptomatic bacteriuria |
4 (1.5) |
4 (1.5) |
8 (1.5) |
|
Catheter site phlebitisc |
5 (1.8) |
3 (1.1) |
8 (1.5) |
|
Infusion site phlebitis |
6 (2.2) |
2 (0.7) |
8 (1.5) |
|
Urinary tract infection |
4 (1.5) |
4 (1.5) |
8 (1.5) |
|
Hypokalemia |
3 (1.1) |
4 (1.5) |
7 (1.3) |
|
Vaginal infection |
1 (0.4) |
6 (2.2) |
7 (1.3) |
|
Alanine aminotransferase increased |
5 (1.8) |
1 (0.4) |
6 (1.1) |
|
Anemia |
2 (0.7) |
4 (1.5) |
6 (1.1) |
|
Aspartate aminotransferase increased |
4 (1.5) |
2 (0.7) |
6 (1.1) |
|
Pyrexia |
4 (1.5) |
2 (0.7) |
6 (1.1) |
|
Dyspnea |
0 |
5 (1.8) |
5 (0.9) |
aTreatment-emergent adverse events are adverse events with a start date and time on or after the first dose of study drug
bFrequency data are for numbers of participants experiencing an event, not for numbers of adverse events
Percentages calculated using the number of patients in the column heading as the denominator
cPhlebitis associated with catheter sites, not with intravenous infusion of study drug
Conclusion
- The study demonstrated noninferiority of meropenem-vaborbactam for the treatment of complicated urinary tract infection
- In patients with complicated UTI, including acute pyelonephritis and growth of a baseline pathogen, meropenem-vaborbactam vs piperacillin-tazobactam resulted in a composite outcome of complete resolution or improvement of symptoms along with microbial eradication that met the noninferiority criterion.
Reference
JAMA. 2018 Feb 27; 319(8): 788–799.












