

Survival Outcomes with Extended and Limited Lymph Node Dissection in Bladder Cancer Patients undergoing Radical Cystectomy



Introduction
The diagnostic role of lymph node dissection (LND) at the time of radical cystectomy (RC) in patients with muscle invasive bladder cancer (BCa) has been established. However, its therapeutic value is yet to be ascertained. There is paucity of data with respect to the optimal anatomic extent of LND and the corresponding therapeutic benefits. The lymphatic landing sites of early metastatic BCa have been described upto the level of inferior mesenteric artery (IMA). However, there are no prospective randomized studies which highlight the oncologic outcome with the extension of LND outside the limited field.
Aim
To evaluate whether there is an improvement in the recurrence free survival (RFS) with an extended LND upto the level of IMA as compared to limited LND in patients with BCa undergoing RC.
Method
Study Design
Prospective randomized phase III study.
Treatment Strategy
- Patients with resectable, histologically confirmed T1G3 or muscle-invasive urothelial BCa were selected
- The cohort was randomized to receive either a limited or extended LND at the time of RC
- LND was performed at bilateral obturator, and internal and external iliac nodes in the limited LND group
- LND was performed at bilateral deep obturator fossa and common iliac nodes as well as presacral, paracaval, interaortocaval and para-aortal nodes upto IMA in addition to all the above sites
- In the limited LND group, removal of at least 4 out of 6 fields as well as resection of 4 or more LNs was mandatory
- In the extended LND group, removal of at least 10 out of 14 LNDs and resection of 12 or more LNs were demanded
Endpoints
Primary Endpoint
- Recurrence-free survival (RFS) defined as time from RC to tumor recurrence or death from BCa
Secondary Endpoints
- Cancer-specific survival (CSS)
- Overall survival (OS)
- Rate of complications
The trial was designed to show 15% advantage of 5-yr RFS by extended LND
Results
- Out of the 401 patients, 203 received limited LND and 198 received an extended LND
- LND was performed as per the protocol in 94% and 87% in the limited and extended LND groups respectively
- The median number of dissected LNs was 19 and 31 in the limited and extended LND groups respectively (p<0.001)
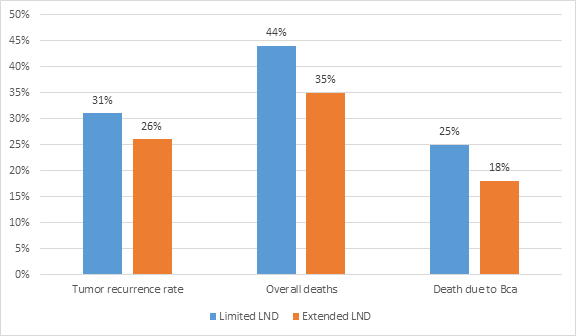
- The overall rate of tumor recurrence and deaths were 29% and 39% respectively
- The comparison between the 2 groups is shown in figure 1.
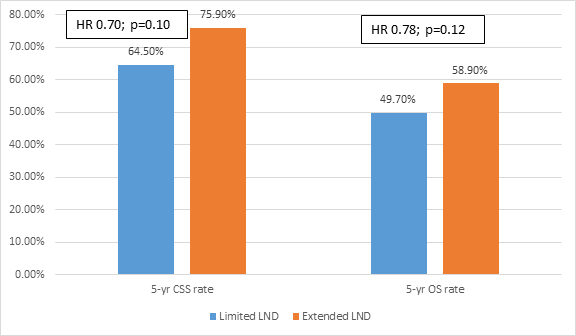
- Extended LND did not show superiority over limited LND with respect to 5-year RFS (64.6% vs 59.2%; HR 0.84, p=0.36)
- The comparison of cancer specific survival rates and overall survival rates are seen in figure 2.
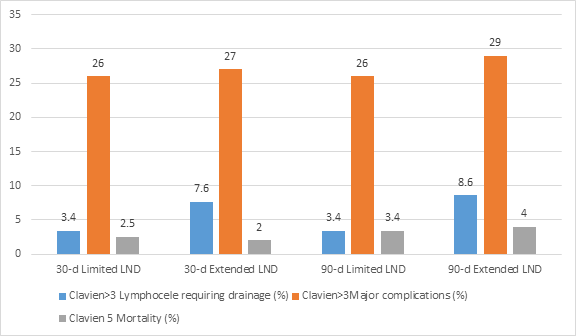
- The 30-day and 90-day mortality rates in the intention-to-treat population were 2.2% and 3.7% respectively
- There were no significant differences in the mortality and major complications after 30 and 90 days postoperatively between the groups as seen in figure 3.
- However, lymphoceles requiring intervention within 90 days postoperatively were more frequent in the extended LND group as seen in figure 3.
- The negative result could be attributed to the inclusion of T1G3 tumors
Conclusion
- The extended lymph node dissection (LND) did not show any significant benefits over limited LND in recurrence-free survival, cancer-specific survival and overall survival
- There were survival differences between the groups but they were statistically insignificant
- A larger trial is warranted to evaluate if extended LND was associated with any clinically significant benefits.
Eur Urol. 2018 Oct 15. Pii: S0302-2838(18)30737-1. Doi: 10.1016/j.eururo.2018.09.047.












