

Six Months vs. Twelve Months of DAPT in Event-Free STEMI Patients after Primary PCI with Second Generation DES



Background
The optimal duration of dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI) with second generation drug-eluting stents (DES) is unclear. Second generation DES have a superior efficacy and safety profile as compared to the first generation DES and bare metal stents. Also, considering the unknown bleeding risk following primary PCI, a shorter DAPT may seem appropriate for patients with ST-elevation myocardial infarction (STEMI) treated with second generation DES
Aim
To evaluate if limiting DAPT to six months in STEMI patients would yield non-inferior clinical outcomes as compared to DAPT for 12 months
Patient Profile
- Patients with STEMI (age 18-85 years) who underwent a primary PCI with the implantation of second generation zotarolimus-eluting stent
- All patients were event-free at six months after primary PCI at the point of randomization (n=870).
Method
Study Design
- Prospective, randomized, multicenter (conducted across 17 study sites in the Netherlands, Norway, Poland, and Switzerland), non-inferiority trial
Interventions
- DAPT comprised of aspirin (loading dose 150-300 mg orally or 250-500 mg intravenously followed by daily oral dose of 75-100 mg) and a P2Y12 inhibitor prasugrel, ticagrelor, or clopidogrel in the following dosage:
- Prasugrel: Loading dose; 60 mg orally followed by oral daily dose of 10 mg
- Patients aged ≥75 years and those weighing less than 60 kg were treated with an initial dose of 60 mg prasugrel orally followed by daily oral dose of 5 mg prasugrel
- Ticagrelor: Loading dose 180 mg orally followed by an oral dose of 90 mg twice daily
- Clopidogrel: Loading dose 600 mg orally followed by oral daily dose of 75 mg
- Patients were randomized 1:1 to single antiplatelet therapy (SAPT) (i.e. aspirin only; 80-100 mg) or to DAPT for an additional six months.
Outcomes
Primary Outcomes
- A patient-oriented composite of all-cause mortality, any myocardial infarction (MI), any revascularization, stroke, and thrombolysis in myocardial infarction (TIMI) major bleeding at 18 months after randomization
Secondary Outcomes
- A composite of all-cause mortality, any MI, stent thrombosis, stroke, and TIMI major bleeding at 18 months follow-up after randomization
Follow-Up
- 18 months (i.e. 24 months after the primary PCI)
Results
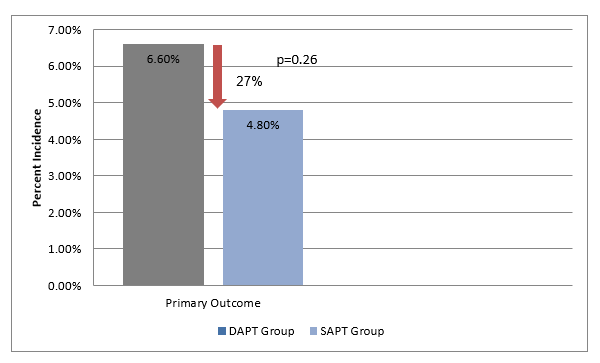
Patients receiving SAPT had an insignificant 27% lower incidence of the primary endpoint as compared to those receiving DAPT (4.8% vs. 6.6%; hazard ratio [HR], 0.73, 95% confidence interval [CI] 0.41 to 1.27; P=0.26) (Figure 1).
- The trial could prove non-inferiority of SAPT vs. DAPT (P=0.004 for non-inferiority), as the upper 95% CI of 1.27 was smaller than the prespecified noninferiority margin of 1.66.
- The incidence of major secondary endpoint, a composite of safety and bleeding at 18 months (i.e. 24 months after the primary PCI), was 3.2% in the SAPT group vs. 4.3% in the DAPT group (hazard ratio 0.75, 95% CI: 0.37 to 1.49; P=0.40).
- There was no significant difference between the SAPT and DAPT groups in terms of the incidence of all-cause mortality, death from cardiac causes; any MI; stent thrombosis; stroke; and TIMI major bleeding (Table 1)
|
Outcome |
SAPT Group |
DAPT Group |
Hazard Ratio (HR) |
95% Confidence Interval |
P value |
|
All-cause mortality |
0.7% |
1.4% |
0.51 |
0.13 to 2.02 |
0.33 |
|
Death from cardiac causes |
0.5% |
0.9% |
0.51 |
0.09 to 2.76 |
0.43 |
|
Any MI |
1.8% |
1.8% |
1.02 |
0.38 to 2.71 |
0.97 |
|
Stent thrombosis |
0.7% |
0.9% |
0.76 |
0.17 to 3.39 |
0.72 |
|
Stroke |
0.7% |
0.7% |
1.02 |
0.21 to 5.03 |
0.99 |
|
TIMI major bleeding |
0.2% |
0.5% |
0.51 |
0.05 to 5.57 |
0.58 |
Conclusions
- Limiting DAPT to six months in STEMI patients who remain event free at six months after primary PCI with second generation DES resulted in non-inferior safety and efficacy outcomes as compared to the currently recommended regimen of 12 months DAPT.
- A shorter DAPT was feasible and safely applicable if clinically required even in patients with STEMI who remain event free for six months after primary PCI.
BMJ. 2018; 363: k3793.











