The liver is a rapidly regenerating organ, and persistent liver injury leads to a process of healing and scar tissue formation resulting in fibrosis, and eventually cirrhosis. The transformation of hepatic stellate cells from vitamin A storage cells to activated hepatic stellate cells which secrete fibrillar collagens is responsible for liver fibrosis following liver injury. Although fibrosis was previously thought to be irreversible and relentlessly progressive, recent studies have challenged these ideas. Treatment of the underlying cause of inflammation has been shown clinically to result in reversal of fibrosis and cirrhosis in patients with liver disease from both viral and non-viral causes.
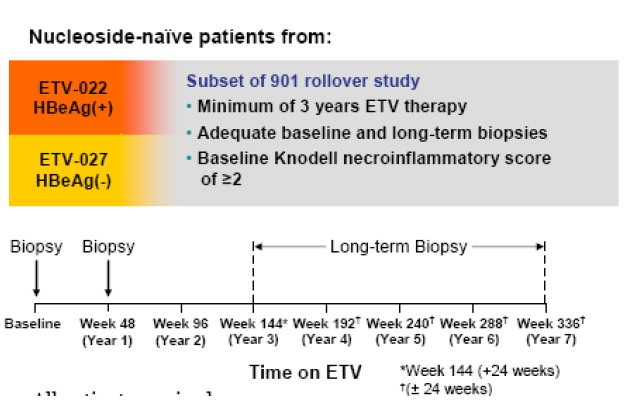
Antiviral therapy for CHB results in the suppression of viral replication, and has been associated with improvement of liver histology in randomized clinical trials. Entecavir is a potent HBV antiviral which demonstrated superior virologic, histologic and biochemical outcomes after 48 weeks of therapy compared to either lamivudine or adefovir in nucleoside-naive patients. The aim of the present study was to determine if long-term treatment with entecavir is associated with continued histologic improvement and reversal of fibrosis or cirrhosis and evaluated nucleoside-naive patients from two Phase III entecavir studies (hepatitis B e antigen (HBeAg)-positive [ETV-022] and HBeAg-negative [ETV-027]) who subsequently entered an open-label rollover study (ETV-901) and received entecavir for a total duration of at least 3 years.