

RECOVERY Trial: Efficacy and Safety of Casirivimab and Imdevimab Combination in Hospitalized COVID-19 Patients



Introduction
Casirivimab and imdevimab are non-competing monoclonal antibodies that bind to two different sites on the receptor binding domain of the SARS-CoV-2 spike glycoprotein, blocking viral entry into host cells
Aim
Randomised Evaluation of COVID-19 Therapy (RECOVERY) trial evaluated the efficacy and safety of casirivimab and imdevimab administered in combination in patients admitted to hospital with COVID-19
Patient Profile
Patients aged at least 12 years admitted to hospital with clinically suspected or laboratory-confirmed SARS-CoV-2 infection
Methods
- Randomised, controlled, open-label platform trial
- 9785 randomly assigned between casirivimab and imdevimab, and usual care
- 4839 assigned casirivimab and imdevimab plus usual care
- 4946 assigned usual care alone
Study Treatment
Patients allocated to the antibody combination received a single dose of casirivimab 4 g and imdevimab 4 g administered together in 250 ml 0·9% saline infused intravenously over 60 min (plus or minus 15 min) as soon as possible after randomisation.
Study Endpoints
- The primary outcome was 28-day all-cause mortality assessed by intention to treat, first only in patients without detectable antibodies to SARS-CoV-2 infection at randomisation (i.e., those who were seronegative) and then in the overall population
- Safety was assessed in all participants who received casirivimab and imdevimab
Results
- 5272 (54%) patients were seropositive at baseline, 3153 (32%) were seronegative, and serostatus was unknown for 1360 (14%)
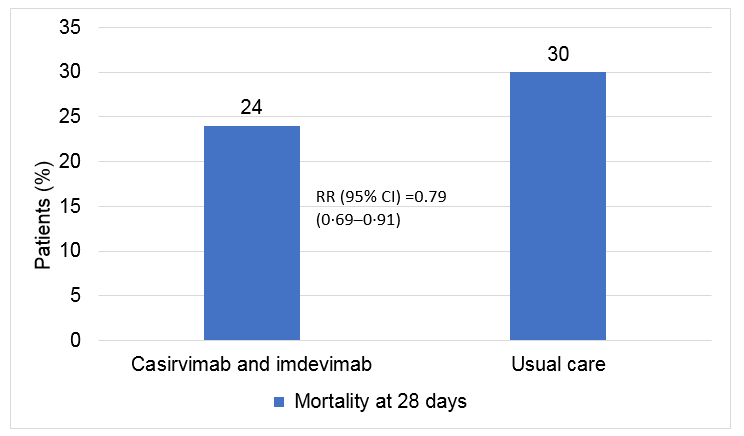
- In patients seronegative at baseline, casirivimab and imdevimab was associated with a significant reduction in the primary outcome of 28-day mortality compared with usual care alone
- Casirivimab and imdevimab was associated with an increased rate of discharge alive from hospital within the first 28 days and a reduced rate of progression to invasive mechanical ventilation or death in seronegative patients
|
|
Casirivimab and imdevimab (n=1633) |
Usual care (n=1520) |
RR |
|
Median duration of hospitalisation, days |
13 (7 to >28) |
17 (7 to >28) |
·· |
|
Discharged from hospital within 28 days |
1049 (64%) |
878 (58%) |
1·19 |
|
Invasive mechanical ventilation or death* |
488/1599 (31%) |
544/1484 (37%) |
0·83 |
|
Invasive mechanical ventilation |
190/1599 (12%) |
202/1484 (14%) |
0·87 |
|
Death |
383/1599 (24%) |
435/1484 (29%) |
0·82 |
|
Subsidiary outcomes |
|
|
|
|
Use of ventilation† |
360/1267 (28%) |
373/1143 (33%) |
0·87 |
|
Non-invasive ventilation |
348/1267 (27%) |
362/1143 (32%) |
0·87 |
|
Invasive mechanical ventilation |
90/1267 (7%) |
120/1143 (10%) |
0·68 |
|
Successful cessation of invasive mechanical ventilation‡ |
10/34 (29%) |
10/36 (28%) |
1·19 |
|
Renal replacement therapy§ |
67/1614 (4%) |
65/1498 (4%) |
0·96 |
Data are n (%), or n/N (%). RR=rate ratios for the outcomes of 28-day mortality, hospital discharge, and successful cessation of invasive mechanical ventilation, and risk ratios for other outcomes. *Excluding patients receiving invasive mechanical ventilation at randomisation. †Excluding patients receiving invasive or non-invasive ventilation at randomisation. ‡Excluding patients not receiving invasive mechanical ventilation at randomisation. §Excluding patients receiving renal replacement therapy at randomisation.
- The proportional effect of casirivimab and imdevimab on mortality differed significantly between seropositive and seronegative patients (p value for heterogeneity=0·002)
|
|
Casirivimab and imdevimab |
Usual care |
RR |
|
Death within 28 days (?21=9·8; p=0·002) |
|
|
|
|
Seronegative |
24% |
30% |
0·79 |
|
Seropositive |
16% |
15% |
1·09 |
|
Unknown |
24% |
24% |
0·97 |
|
All participants |
19% |
21% |
0·94 |
|
Discharge alive from hospital (?21=17·2; p<0·001) |
|
|
|
|
Seronegative |
64% |
58% |
1·19 |
|
Seropositive |
75% |
77% |
0·94 |
|
Unknown |
63% |
64% |
0·96 |
|
All participants |
70% |
69% |
1·02 |
|
Invasive mechanical ventilation or death (?21= 12·5; p<0·001) |
|
|
|
|
Seronegative |
31% |
37% |
0·83 |
|
Seropositive |
19% |
17% |
1·10 |
|
Unknown |
29% |
28% |
1·05 |
|
All not on invasive mechanical ventilation at randomisation |
24% |
25% |
0·97 |
- There were no deaths attributed to the treatment, or meaningful between-group differences in the pre-specified safety outcomes of cause-specific mortality, cardiac arrhythmia, thrombosis, or major bleeding events
- In the overall study population frequency of fever (in 79 [4%] of 1792 vs 52 [3%] of 1715), sudden hypotension (66 [4%] vs 39 [2%]), and thrombotic events (31 [2%] vs 24 [1%]) was numerically higher in the casirivimab and imdevimab group versus the usual care group, and the frequency of sudden worsening in respiratory status (369 [21%] vs 372 [22%]) and clinical haemolysis (26 [1%] vs 31 [2%]) was numerically lower
- Serious adverse reactions reported in seven (<1%) participants were believed by the local investigator to be related to treatment with casirivimab and imdevimab
Conclusion
- In patients admitted to hospital with COVID-19, the monoclonal antibody combination of casirivimab and imdevimab reduced 28-day mortality in patients who were seronegative (and therefore had not mounted their own humoral immune response) at baseline but not in those who were seropositive at baseline
- The results support the use of the monoclonal neutralising antibody combination of casirivimab and imdevimab in seronegative patients admitted to hospital with COVID-19 caused by SARS-CoV-2 variants that are sensitive to these antibodies
Reference
Lancet 2022; 399: 665–76












