

Preservation of Beta-cell Function: Daily Metformin vs. Intermittent Intensive Insulin Therapy



Background
Type-2 diabetes mellitus (T2DM) is characterized by a progressive decline of pancreatic beta cell function that leads to loss of glycaemic control and this creates a need for intensification of antihyperglycemic therapy. Short course of intensive insulin therapy (IIT) has shown to improve reversible beta-cell dysfunction and thereby induce diabetes remission. However, these effects are temporary as beta cell function deteriorates over time after the therapy is stopped.
Aim
To evaluate the impact of a short induction IIT followed by a maintenance therapy of either daily metformin or intermittent short term insulin therapy every 3 months on beta cell function and glycaemic control over 2 years.
Patient Profile
- T2DM patients (≤5 year duration, age: 30-80 years) treated with metformin or lifestyle modification only (n=24).
- Screening HbA1c: 6.0%-9.5% (in case patients did not receive any antidiabetic medications) or 5.5%-9.0% (in case patients were treated with metformin)
Method
Study Design
- The REmission Studies Evaluating Type 2 Diabetes- Intermittent Insulin Therapy Pilot (RESET IT Pilot) was an open label, parallel arm, randomized controlled trial
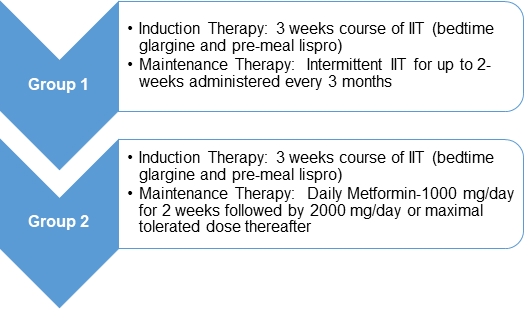
Treatment Strategy
Assessments
- Serial assessment of glucose homeostasis using oral glucose tolerance test (OGTT) at baseline, after induction IIT, and every 3-months thereafter during the 2-year maintenance phase.
Outcomes
Primary Outcome
- Assessment of beta cell dysfunction measured by Insulin Secretion Sensitivity Index-2 (ISSI-2) at the end of 2 years
Secondary Outcomes
- Baseline adjusted HbA1c
- Fasting glucose levels and different measures of beta cell function such as C- peptide concentration and insulin secretion rate
Results
- The patients enrolled in this study had a mean diabetes duration of 2 years and a mean HbA1c of 6.4%
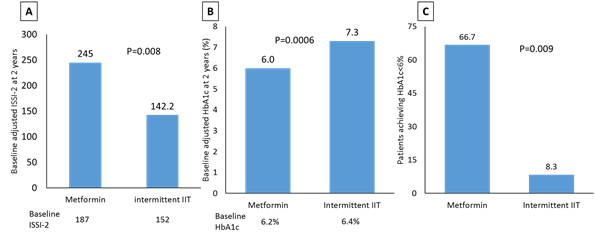
- The ISSI-2 (a measure of beta-cell function) was significantly higher in metformin group compared to intermittent IIT group (245 vs. 142.2, p=0.008) at 2 years (Figure 1A)
- As compared to intermittent IIT, metformin therapy showed significantly lower HbA1c (7.3% vs. 6.0%, p=0.006; Figure 1B) and fasting glucose levels (136.8 vs. 102.6 mg/dL, p= 0.0002)
- More number of patients had HbA1c ≤6% in metformin group compared to intermittent IIT group (66.7% vs. 8.3%, p=0.009; Figure 1C)
- None of the patients in metformin group had loss of glycaemic control (HbA1c> 8.0% on 2 consecutive assessments) whereas 41% of patients in intermittent IIT group had a loss of glycaemic control, over 2 years
- No difference in insulin sensitivity between the two groups was observed; this suggests that the improvement in glycaemic control is attributable to improvement in beta-cell function
- This glycaemic control was achieved without any increased risk of hypoglycaemia or other adverse events
Conclusion
- In early type-2 diabetes patients who undergo short-term initial intensive insulin therapy, maintenance therapy with metformin is superior to intermittent intensive insulin therapy for preservation of beta cell function and glycaemic control for over 2 years.
Diabetes Obes Metab. 2018 (Published Online); doi: 10.1111/dom.13236.












