

Prasugrel Renders Superior Efficacy vs. Ticagrelor in ACS Patients Undergoing Invasive Evaluation

4 Oct, 19


Background
Patients with acute coronary syndrome (ACS) are treated with dual antiplatelet therapy (DAPT) as a part of standard treatment. Use of prasugrel or ticagrelor is preferred over clopidogrel due to their rapid onset of action and consistent platelet inhibition. Nevertheless, little is known about the relative merits of ticagrelor vs. prasugrel in ACS patients for whom invasive evaluation is planned.
Aim
To compare the efficacy and safety of ticagrelor vs. prasugrel in ACS patients for whom invasive evaluation was planned
Patients Profile
- Patients hospitalized for ACS [ST-segment elevation myocardial infarction (STEMI), non–ST-elevation myocardial infarction (NSTEMI), or unstable angina] for whom invasive evaluation (angiography) was planned (n=4018)
Methods
Study Design
- Multicenter (23 centers across two countries), randomized, open-label, phase-4 trial
Treatment Strategy
- Patients were randomized 1:1 as follows:
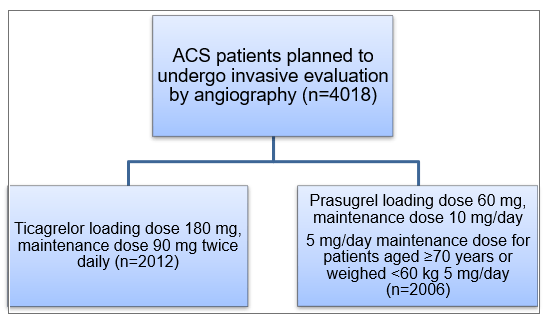
- Ticagrelor therapy was initiated at a loading dose of 180 mg and continued at a maintenance dose of 90 mg twice daily. Patients assigned to ticagrelor received the loading dose as soon as possible after randomization.
- Amongst patients treated with prasugrel, timing of the initiation of the trial drug was influenced by the clinical presentation. Patients with STEMI received prasugrel as soon as possible after randomization. Amongst ACS patients without ST-segment elevation, administration of prasugrel loading dose was postponed until the coronary anatomy was known (no pretreatment before diagnostic angiography) and before proceeding to PCI.
Outcomes
Primary Outcome
- Composite of death, MI, or stroke at one year
Secondary Outcomes
- Safety end point: Incidence of bleeding (BARC type 3-5) at one year
- Incidence of the individual components of the primary end point at one year, and the incidence of definite or probable stent thrombosis at one year
Follow-up Visits
- 30 days, six months and one year
Results
- At admission, 41.1% patients had a suspected diagnosis of STEMI, 46.2% of NSTEMI and 12.7% of unstable angina..
- The incidence of primary outcomes was significantly higher amongst patients receiving ticagrelor vs. those receiving prasugrel [9.3% vs. 6.9%, hazard ratio (HR); 1.36; 95% confidence interval (CI), 1.09 to 1.70; P = 0.006] (Figure 1). The same was also true for the incidences of the individual components of the primary outcome (Table 1).
Figure 1: Incidence of Primary outcomes in the study groups
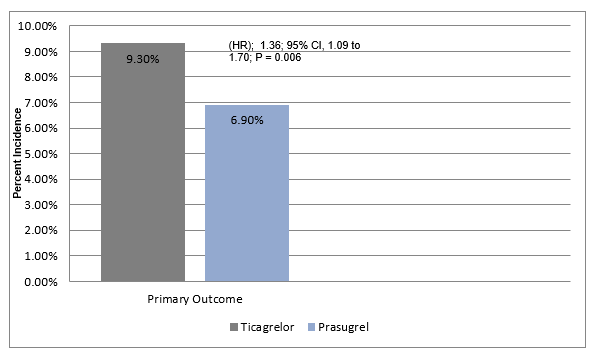
Table 1: Incidence of individual component of primary outcome in the study groups
|
Endpoint |
Ticagrelor |
Prasugrel |
HR |
|
Death |
4.5% |
3.7% |
1.23 |
|
MI |
4.8% |
3.0% |
1.63 |
|
Stroke |
1.1% |
1.0% |
1.17 |
- Definite or probable stent thrombosis occurred in 1.3% of patients assigned to ticagrelor and 1.0% of patients assigned to prasugrel, and definite stent thrombosis occurred in 1.1% and 0.6%, respectively.
- Incidence of major bleeding [as defined by the Bleeding Academic Research Consortium (BARC) scale] with prasugrel was not higher than that seen with ticagrelor (4.8% vs. 5.4%, HR; 1.12; 95% CI, 0.83 to 1.51; P = 0.46).
Conclusion
- Prasugrel-based antiplatelet strategy rather than ticagrelor-based antiplatelet strategy rendered greater protection against a composite of death, MI and stroke at one year in ACS patients with or without STEMI who were scheduled for an invasive evaluation.
- These benefits of prasugrel were not at a cost of increased incidence of major bleedings.
New Engl J Med. Sep 1, 2019 (Published Online); DOI: 10.1056/NEJMoa1908973.

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


