

PIONEER-HF: Efficacy and Safety of Sacubitril/Valsartan in ADHF Patients as per the Dose Level Achieved



Introduction
In-hospital initiation and continuation of sacubitril/valsartan rather than enalapril is not only well tolerated, but also associated with a greater reduction in N-terminal pro–B-type natriuretic peptide (NT-proBNP), and reduced risk of cardiovascular (CV) death or rehospitalization for HF through 8 weeks in patients hospitalized for acute decompensated heart failure (ADHF). Nevertheless, all patients do not achieve the target dose of sacubitril/valsartan, and the benefits of sacubitril/valsartan administered below the target dose have not been established as of yet.
Aim
To evaluate the efficacy and safety of sacubitril/valsartan as per the dose level achieved in the PIONEER-HF (Comparison of Sacubitril/Valsartan Versus Enalapril on Effect on NT-proBNP in Patients Stabilized From an Acute Heart Failure Episode) trial.
Patient Profile
- Patients (age ≥18 years; n=881) with reduced ejection fraction (EF) (left ventricular EF [LVEF] ≤40% and an NT-proBNP ≥1600 pg/ml or a B-type natriuretic peptide (BNP) ≥ 400 pg/ml
- All patients had a primary diagnosis of ADHF, including signs and symptoms of fluid overload.
- The enrollment period for patients ranged from no less than 24 hours up to 10 days after initial presentation to the hospital (median; 68 hours), while they were still hospitalized.
- Patients were hemodynamically stable (defined as; maintenance of a systolic blood pressure [SBP] of ≥100 mm Hg for the preceding 6 hours, with no increase in the dose of intravenous [IV] diuretics and no use of IV vasodilators during the preceding 6 hours and no use of IV inotropes during the preceding 24 hours) before randomization.
Methods
Study Design
- A subgroup analysis of the PIONEER HF trial
- PIONEER HF was a multicenter, randomized, double-blind, active-controlled trial conducted across 129 sites in the US
Treatment Strategy
- Post-washout period of 36 hours, patients were randomized to sacubitril/valsartan (n=440; initial dose: 24 / 26 mg or 49/ 51 mg twice daily) or enalapril (n=441:2.5 mg or 5 mg twice daily)
- The study medications were up-titrated as follows to achieve a target dose of 97/103 mg twice daily for sacubitril/valsartan or 10 mg twice daily for enalapril:
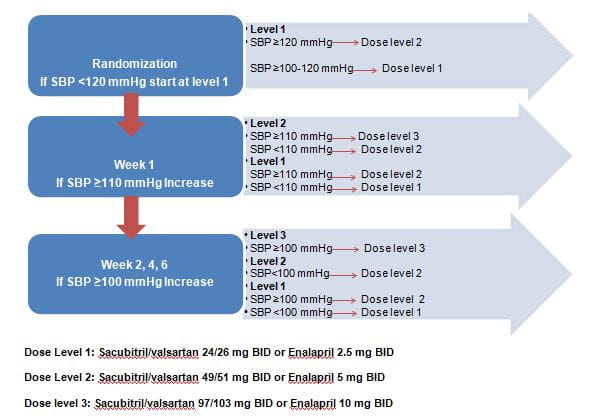
Outcomes
- This analysis assessed the following patient outcomes as per the dose level achieved at week 4 post-randomization
Efficacy Outcomes
- The time-averaged proportional change in the NT proBNP from baseline through week 8
- The composite of rehospitalization for HF or CV death
Safety Outcomes
- Incidence of worsening renal function (defined as an increase in the serum creatinine concentration of ≥0.5 mg/dl and a decrease in the estimated glomerular filtration rate of ≥25% from baseline)
- Incidence of hyperkalemia (serum potassium concentration of ≥5.5 mmol/l)
- Incidence of symptomatic hypotension
Results
- At week 4, post-randomization, 57% patients achieved target dose (55% patients on sacubitril/valsartan and 60% patients on enalapril), 24% received dose level 2 and 19% received dose level 1. As per a multivariable analysis, older age, lower baseline SBP, and white race were the significant predictors of not attaining the target dose by week 4 post-randomization.
- The baseline characteristics did not differ between the two treatment groups within each dose level.
- The proportion of NT-proBNP reduction remained consistent at week 8 regardless of the dose level, with sacubitril/valsartan providing superior reductions as compared to enalapril (overall hazard ratio [HR]; 0.72; pinteraction, 0.67; Fig 1).
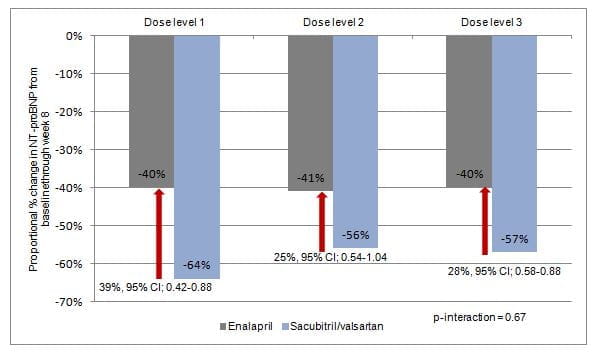
- Greater reductions in NT-proBNP concentrations with sacubitril/valsartan vs. enalapril were evident right from the beginning, and throughout the study even in the patients in whom the dose was not escalated beyond dose level 1.
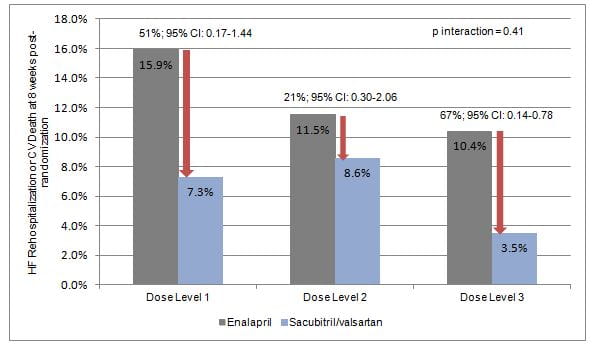
- There was a consistent reduction in rehospitalization for HF or CV death with sacubitril/valsartan vs. enalapril regardless of the dose level achieved at week 4 (overall HR; 0.58, 95% CI; 0.39-0.87, pinteraction=0.41; Fig 2)
- There was no heterogeneity across dose levels in the effect of sacubitril/valsartan with respect to the pre-specified adverse events (worsening renal function or hyperkalemia) through 8 weeks.
- Patients achieving submaximal doses of the study drug had higher overall rates of symptomatic hypotension regardless of treatment group, nevertheless; the risk of symptomatic hypotension did not differ significantly with sacubitril/valsartan vs. enalapril across dose levels. In fact, a non-significant trend toward more frequent symptomatic hypotension with sacubitril/valsartan was evident only in patients achieving dose level 3
Conclusions
- Amongst hemodynamically stabilized patients with ADHF, sacubitril/valsartan exhibited generally consistent efficacy and safety across various dose levels.
- The findings support the in-hospital initiation and continued post-hospitalization use of sacubitril/valsartan broadly, including in patients who may not tolerate early up-titration to the target dose.
J Am Coll Cardiol HF 2020; 8:834–43.












