

OPTIMISE Trial: Impact of Antihypertensive Medication Reduction in Elderly Hypertensive Patients

7 Jul, 20


Background
Studies have suggested that lower blood pressure (BP) and multiple antihypertensive prescriptions may have a detrimental effect in some elderly patients with polypharmacy and multimorbidity. Reducing medications is recommended in this patient subgroup when the benefits of continued treatment may not outweigh the harm. Nevertheless, there is no evidence to guide medication reduction in these patients.
Aim
The Optimising Treatment for Mild Systolic Hypertension in the Elderly (OPTIMISE) study evaluated the possibility of reducing antihypertensive medication without significant changes in systolic blood pressure (SBP) control or adverse events during a 12-week follow-up.
Patient Profile
Inclusion Criteria
- Patients (age ≥ 80 years; n=569) whose primary care physician considered them appropriate for antihypertensive medication reduction
- All patients had SBP < 150 mmHg, and were receiving at least 2 antihypertensive medications for at least 12 months
Exclusion Criteria
- Patients with a history of heart failure due to left ventricular dysfunction or myocardial infarction or stroke in the preceding 12 months, and patients with secondary hypertension
Methods
Study Design
- A randomized, unblinded, parallel-group, non-inferiority trial conducted across 69 primary care sites in England
Treatment Strategy
- Participants were randomized 1:1 as follows:
- Intervention group: A strategy of antihypertensive medication reduction (removal of 1 drug, n = 282)
- Control group: Usual care (no medication changes were mandated, n = 287)
- Amongst the patients with antihypertensive medication reduction, the treatment was reinstated if SBP was above 150mmHg or diastolic blood pressure (DBP) was above 90 mm Hg for more than a week, adverse events occurred, or signs of accelerated hypertension developed.
Outcomes
Primary Outcome
- The relative risk (RR) of SBP control (< 150 mmHg) at 12-week follow-up (prespecified non-inferiority margin for RR; 0.90)
Secondary Outcomes
- Proportion of participants maintaining medication reduction
- Between group differences in BP, frailty, quality of life, adverse effects, and serious adverse events
Follow-up
- 12 weeks
Results
- Mean age of the study population was 84.8 years; 48.5% (n= 276) were women. Patients were prescribed median of 2 antihypertensive medications at baseline, the trial was completed by 93.8% (n=534) patients.
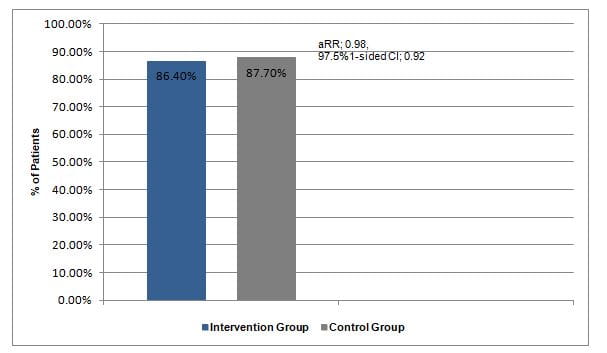
- Similar proportion of patients in the intervention group and the control group achieved SBP <150 mmHg at 12 weeks (86.4% vs. 87.7%, adjusted RR [aRR]; 0.98, 97.5%1-sided CI; 0.92 to ∞) (Figure 1).
Figure 1: Proportion of patients achieving SBP <150 mmHg at 12 weeks
- With respect to the 7 prespecified secondary outcomes, 5 did not differ significantly in both the study groups.
- Mean SBP changed from 129.4 mmHg at baseline to 133.7 (95% CI, 131.7 to 135.6) mmHg at week 12 in the intervention group and from 130.5 mmHg at baseline to 130.8 (95%CI, 128.9 to 132.7) mmHg at week 12 in the control group. This indicated that change in SBP at 12 weeks was 3.4 mmHg (95% CI, 1.0 to 5.8 mmHg) higher in the intervention group vs. the control group after correcting for baseline BP.
- Mean DBP changed from 68.4 mmHg at baseline to 70.9 (95% CI, 69.6 to 72.1) mmHg in the intervention group and 70.1 mmHg at baseline to 69.7 (95% CI, 68.5 to 70.8) mmHg in the control group. The adjusted mean difference in change in DBP corrected for baseline was 2.2 mmHg (95%CI, 0.9 to 3.6 mmHg).
- At 12 weeks, the medication reduction was sustained in 66.3% (n=187) patients.
- There was not much difference in the frailty, quality of life, or adverse effects at follow-up in both the study groups. The incidence of at least 1 serious adverse event was higher in the intervention vs. the control group (4.3% vs. 2.4%; aRR, 1.72; 95%CI, 0.7 to 4.3).
Conclusions
- Among elderly patients treated with multiple antihypertensive medications, a strategy of medication reduction was non-inferior to usual care strategy with regards to SBP control at 12 weeks.
- Antihypertensive medication reduction may not be associated a substantial change in BP control in some elderly hypertensive patients. Further research is warranted to explore the associated long-term clinical outcomes.
JAMA. 2020;323(20):2039-2051.
Related Topics
More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


