

Non-Inferiority of Degarelix with Goserelin in Chinese Men with Prostate Cancer



Introduction
The incidence and mortality of prostate cancer (PCa) is significant in Asia. Androgen deprivation therapy (ADT) using gonadotropin releasing hormone (GnRH) agonists or GnRH antagonists is well established modality for the treatment of PCa. Exacerbation of clinical symptoms is possible due to delayed response and testosterone surges with GnRH agonists. GnRH antagonists are associated with reversible medical castration due to rapid testosterone suppression without testosterone surges. The clinical efficacy and safety of degarelix, a 3rd generation GnRH antagonist has been demonstrated in the western population evidenced as regulatory approval in US, EU and Japan. However, confirmatory studies conducted in Asian population are scarce.
Aim
This study assessed whether degarelix was non-inferior to goserelin in suppressing and maintaining castrate testosterone levels from Day 28 to Day 364 in Chinese patients with prostate cancer.
Method
Study Design
- Open-label, multi-center, randomized, parallel-group study
Treatment Strategy
- Men aged ≥18 years with a histologically confirmed adenocarcinoma of the prostate (all stages), prostate-specific antigen (PSA) level ≥2.0 ng/mL at screening, testosterone level >1.5 ng/mL, and life expectancy of >1 year were included in this study.
- Cohort was randomized in a 1:1 ratio to receive once-a-month subcutaneous injection of either degarelix or goserelin with 28-day intervals for 12 months
- Degarelix was administered as a deep subcutaneous (s.c.) injection in the abdominal region, at a starting dose of 240 mg (40 mg/mL) at Day 0, followed by 12 monthly maintenance doses of 80 mg (20 mg/mL).
- Goserelin 3.6 mg sustained-release depot was administered s.c. into the anterior abdominal wall as 12 monthly doses.
Endpoints
Primary Endpoint
- Difference in 1-year cumulative probability of suppressing testosterone to ≤0.5 ng/mL from day 28 to day 364. Non-inferiority was to be established if the lower 95% confidence interval (CI) limit for difference in cumulative probability between the treatment arms was greater than −10%.
Secondary Endpoints
- From day 56 to day 364:
- Cumulative probabilities of testosterone at castrate levels
- PSA-progression-free-survival (PSA-PFS): An endpoint defined as PSA failure, death or any additional treatment given – whichever occurs earlier
- PFS
- Quality of life as measured by EORTC QLQ instrument and question 8 of the IPSS
- Severity of LUTS as measured by IPSS
- Cumulative probabilities of testosterone at castrate levels at day 3 and at subsequent visit
- Adverse events (AEs)
Results
- Baseline demographics and disease characteristics were similar between the 2 groups
- Out of the overall cohort of 285 patients, 239 completed the study degarelix (n=123) and goserelin (n=116)
- Degarelix was non-inferior to goserelin in achieving and maintaining serum testosterone suppression at castrate levels from Day 28 to Day 364.
- The difference between the two treatment groups was 3.6% (95% CI: −1.5%, 8.7%), and the lower limit of the CI (for the difference in probability) was higher than the pre-defined threshold of > −10%
- The primary endpoint was achieved by 97% in the degarelix group as compared to 93.4% in the goserelin group
- The comparison of secondary efficacy endpoints is shown in figure 1.
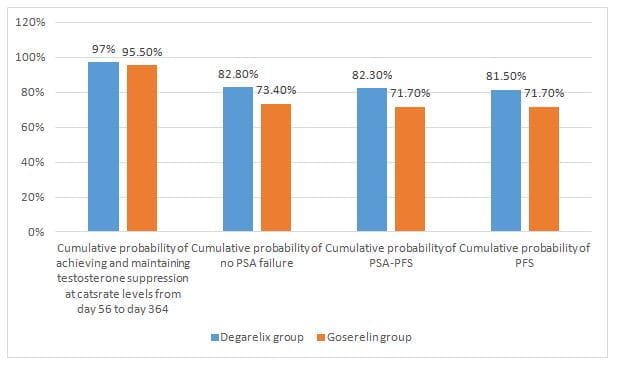
- The cumulative probability of PSA-PFS at Day 364 was higher for degarelix as seen in figure 1 (p=0.038).
- Rapid suppression of testosterone levels to castrate levels was attained by 96% in degarelix group (0.25 ng/mL) at Day 3 compared with none in goserelin group which experienced a 53% increase (p<0.0001)
- More rapid and profound PSA reduction from baseline to day 3 was reported in the degarelix arm (22.2% vs 8.65%)
- The health-related quality of life in both arms of the trial was comparable
- Degarelix tended to reduce severity of LUTS similarly or more as compared to goserelin as measured by IPSS (Reduction of 5.92 vs 5.24 points respectively).
- The incidence of treatment-emergent AEs was higher in degarelix arm (76.1% vs 58.9%) with more injection site reactions (ISRs) with degarelix (52.1%) versus goserelin (8.5%).
- The proportion of ISRs was higher with loading dose injection (35%) vs maintenance dose injections (29%).
- Degarelix was associated with a better safety profile as compared to goserelin as regards cardiac and musculoskeletal / connective tissue disorders (7.7% vs 10.6% respectively in both cases).
- The discontinuation rates were 2.8% and 6.4% in the degarelix and goserelin groups, respectively.
- However, none of these were assessed as treatment-related and none of the discontinuations were due to injection site reactions.
Conclusions
- Degarelix was non-inferior to goserelin in achieving and maintaining testosterone suppression at castrate levels with an acceptable safety profile during 1-year treatment in the Chinese patients with prostate cancer.
- Treatment with degarelix resulted in improved disease control, indicated by significantly higher prostate-specific antigen progression-free survival (PSA-PFS).
- Both treatments were well tolerated by the patients.
Asian J Urol. 2020 Jul;7(3):301-8. Doi: 10.1016/j.ajur.2019.09.003.












