

Indian Prospective Study Comparing the Nephrotoxicity of Colistin and Polymyxin B Administered in Currently Recommended Doses



Introduction
Polymyxins have been associated with a risk of nephrotoxicity. Different studies have evaluated the toxicity of polymyxins and have demonstrated a wide variation in the rates of nephrotoxicity. However, there are no prospective studies which have compared the nephrotoxicity of colistin and polymyxin B when they are administered in high doses and as per current recommendations.
Aim
The current study was conducted to compare the nephrotoxicity of colistin and polymyxin B when used at optimum doses and explore the associated risk factors in the Indian population
Methods
Study Design
Prospective, observational study conducted from July 2016 to June 2017 in an Indian tertiary care hospital.
Patient Profile
Inclusion Criteria
- Adult patients admitted to intensive care units (ICU) who received intravenous (IV) colistin (n=61) or polymyxin B (n=51) for more than 48 hrs. The patients in two groups of study were similar in baseline demographics, comorbidities, acute physiology and chronic health evaluation (APACHE 2) score and baseline creatinine clearance.
- Overall, in all these patients (N=112), the site of infection was lungs in 66 (58.9%), urinary tract in 19 (17.0%), blood stream in 10 (8.9%) and abdomen in 9 (8.0%) patients. The pathogens were isolated in 77 (68.7%) patients and include Klebsiella (27.7%), Pseudomonas (17.0%), Acinetobacter (19.6%) and E. coli (4.5%). There was no growth on cultures in 35 (31.2%) patients.
- The patients in colistin (COL) and polymyxin (PMB) groups had a mean estimated creatinine clearance of 60.8+33.5 and 55.4+31.6 mL/min respectively.
Exclusion Criteria
Patients who-
- had baseline chronic kidney disease (CKD) on hemodialysis or baseline creatinine clearance <10 mL/min.
- showed fluctuating renal parameters such as changes in serum creatinine >50% from baseline prior to initiation of polymyxins.
- received intravenous contrast.
- are receiving any other nephrotoxic drug like aminoglycosides, vancomycin, amphotericin B, NSAIDs, cyclosporine, etc.
- received significant doses of diuretics such as furosemide >20 mg or torsemide >10 mg over 24 hrs.
Treatment Strategy
- The choice of drug was left to the discretion of the treating physician.
- All patients in both colistin and polymyxin groups received a loading dose.
- The dosing schedule for patients receiving colistin was based on the ideal body weight and creatinine clearance as shown in table 1.
|
Renal function |
Loading dose |
Maintenance dose (12 hrs after loading dose) |
|
Normal renal function or creatinine clearance >50 mL/min |
5 mg/kg (or 1,50,000 U/kg) IV over 40-60 min
|
2.5 mg/kg (or 75,000 U/kg) IV twice daily |
|
Creatinine clearance 20-50 mL/min |
2.5 mg/kg (or 75,000 U/kg) IV once daily | |
|
Creatinine clearance <20 mL/min |
2.5 mg/kg (or 75,000 U/kg) IV on alternate days | |
|
Patient on hemodialysis |
Additional dose of 50 mg (or 15,00,000 U) post dialysis |
- The dosing schedule for patients receiving polymyxin B was based on actual body weight and there was no dose modification for reduced creatinine clearance. Due to the polymyxin B’s poor penetration in urinary tract, it was not used in suspected or confirmed cases of urinary tract infection (UTI),
- The polymyxin B group received loading dose of 2.5 mg/kg as 2 hrs IV infusion followed by maintenance dose of 1.5 mg/kg as 1 hr IV infusion twice daily, started 12 hrs after loading dose.
- Median colistin dose was 233.3 [inter quartile range (IQR) 150–300] mg/day and median polymyxin B dose was 200 (IQR 180–240) mg/day.
- Median duration of colistin and polymyxin B use was 7 (IQR 5–7) days and 7 (IQR 7–9) days respectively.
Endpoints
- Nephrotoxicity or renal failure was defined as twofold increase in serum creatinine or 50% decrease in estimated baseline creatinine clearance.
- Serum creatinine levels were measured daily for a minimum of 7 days after the course of drugs was over.
- Return of serum creatinine to ≤ 2 times of baseline creatinine or greater than 50% of baseline creatinine clearance was defined as reversal of nephrotoxicity.
- The association of different variables with nephrotoxicity such as age, body mass index (BMI), (APACHE 2, diabetes mellitus (DM), and dose was also analyzed.
- For all the statistical tests, the significance level was 5%.
Results
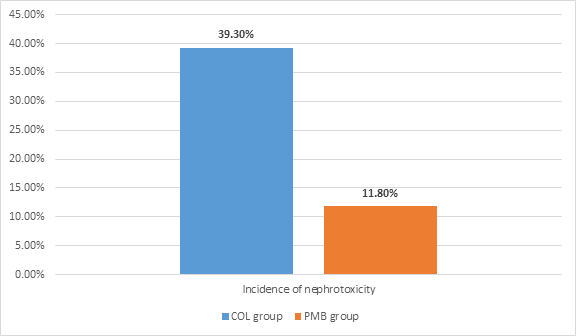
- Overall, the incidence of nephrotoxicity in all patients was 26.8%.
- The incidence of nephrotoxicity was significantly higher in the COL group compared to PMB group (P=0.001) as shown in figure 1.
- The incidence of renal failure as per the first three parameters of RIFLE (Risk, Injury, Failure, Loss of kidney function and End-stage kidney disease) criteria was higher in the COL group (52.4%) than in the PMB group (19.6%) (P<0.001).
- The comparison of other outcomes are demonstrated in table 2.
|
Outcomes |
COL group |
PMB group |
|
Mean onset of renal failure |
3.8+0.8 days |
4.2+0.7 days |
|
Mean duration of kidney injury |
4.9+3.1 days |
5.0+2.4 days |
|
% patients required hemodialysis and drug discontinuation |
14.8% |
2% |
|
% patients with reversal of nephrotoxicity at the end of week 1 after the completion of therapy |
75% |
83.3% |
|
% patients with renal failure at the end of week 1 after the completion of therapy |
9.8% |
2% |
- The incidence of renal failure in the COL group was significantly higher (63%) in patients who received a daily dose of >300 mg (or ≥ 9 million international units) (P=0.001, OR 6.56).
- The subgroup analysis of COL group revealed that the incidence of renal failure was less in patients with low baseline creatinine clearance of <50 mL/min (17.9%) than that in patients with creatinine clearance >50 mL/min (57.6%) (P=0.002). This difference in nephrotoxicity can, thus, be attributed to dose as the patients with lower creatinine clearance received less daily dose of colistin (150 mg, IQR 150– 233.3), compared to those with higher creatinine clearance (300 mg, IQR 291.6–333.3) (P < 0.05).
- Diabetes, age or BMI did not have any effect on colistin toxicity.
- There was higher incidence of renal failure in COL group patients with lower APACHE 2 score (14 of 27, 51.9%) compared to higher APACHE 2 score (10 of 34, 29.4%), although this was not statistically significant (P = 0.075). This was also due to the fact that patients in higher APACHE group received lower colistin dose (233.3 mg, IQR 191.6–283.3) compared to patients in lower APACHE group (300 mg, IQR 166.7–308.3).
- Out of the 6 (11.8%) patients in PMB group who developed nephrotoxicity, 5 patients (83.3%) had baseline renal dysfunction, i.e. creatinine clearance < 50 mL/min. There was no effect of any other factor on polymyxin B nephrotoxicity.
Conclusion
- In terms of the currently recommended doses, the nephrotoxicity associated with colistin was significantly higher than that with polymyxin B in patients admitted to intensive care unit (ICU).
- However, colistin toxicity was dose dependent, mostly mild to moderate and reversible.
Ann Clin Microbiol Antimicrob. 2018;17(1):15. Doi: 10.1186/s12941-018-0262-0.











