

Impact of Sacubitril-Valsartan Treatment on Patients Hospitalized for Acute Decompensated HF



Background
More than 1 million hospitalizations in the United States (US) are annually attributed to acute decompensated heart failure (HF). It is yet not known whether initiation of sacubitril–valsartan therapy would be safe and effective among patients hospitalized for acute decompensated HF.
Aim
PIONEER-HF (Comparison of Sacubitril–Valsartan versus Enalapril on Effect on NT-proBNP in Patients Stabilized from an Acute Heart Failure Episode) trial assessed the efficacy and safety of initiation of sacubitril–valsartan vs. enalapril, in hemodynamically stabilized patients, hospitalized for acute decompensated HF.
Patient Profile
- Patients (age ≥18 years; n=881) with reduced ejection fraction (EF) (left ventricular EF [LVEF] ≤40% and an N-terminal pro–B-type natriuretic peptide (NT-proBNP) ≥1600 pg/ml or a B-type natriuretic peptide (BNP) ≥ 400 pg/ml.
- All patients had a primary diagnosis of acute decompensated HF, including signs and symptoms of fluid overload.
- The enrollment period for patients ranged from no less than 24 hours up to 10 days after initial presentation to the hospital (median; 68 hours), while they were still hospitalized.
- Patients were hemodynamically stable (defined as; maintenance of a systolic blood pressure of ≥100 mm Hg for the preceding 6 hours, with no increase in the dose of intravenous [IV] diuretics and no use of IV vasodilators during the preceding 6 hours and no use of IV inotropes during the preceding 24 hours) before randomization.
Methods
Study Design
- A multicenter, randomized, double-blind, active-controlled trial conducted across 129 sites in the US.
Treatment Strategy
- A washout period of 36 hours was ensured before initiating the sacubitril/valsartan treatment.
- Patients were randomized as follows (refer fig 1pg 5)
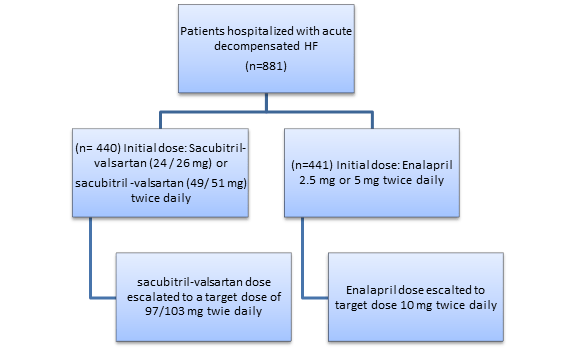
- All the patients were monitored for a minimum of 6 hours after the administration of the third dose before discharge from the hospital.
Follow-up Visits
- Week 1, 2 and every 2 weeks thereafter
Outcomes
Primary Efficacy Outcome
- The time-averaged proportional change in the NT proBNP from baseline through weeks 4 and 8
Key Safety Outcome
- Worsening renal function (an increase in the serum creatinine concentration of ≥0.5 mg/dL and a decrease in the estimated glomerular filtration rate [eGFR] ≥25%)
- Hyperkalemia (a serum potassium concentration of ≥5.5 mmol/L)
- Symptomatic hypotension
- Angioedema
Secondary Efficacy Outcome
- The time-averaged proportional changes in the high-sensitivity troponin T (Hs-TnT) concentration, BNP concentration, and ratio of BNP to NT-proBNP
Trial Duration
8 weeks
Results
- Mean age of the study population was 61 years, 72.1% were male, and 35.9% were black. Nearly 52.1% (n=459) patients were not receiving treatment with an angiotensin converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB).
- By week 8, 55.2% (n=243) patients in the sacubitril-valsartan group and 60.8% (n=268) in the enalapril group were receiving the target dose of the assigned drug.
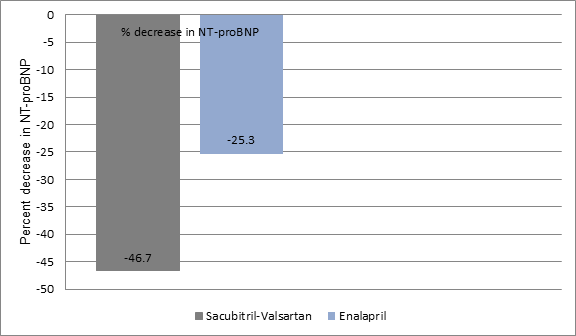
- Patients in the sacubitril-valsartan group had a significantly greater decrease in the NT-proBNP concentrations as compared to the patients treated with enalapril.
- The ratio of the geometric mean of values achieved at weeks 4 and 8 as against the baseline value was 0.53 vs. 0.75 in the sacubitril–valsartan vs. enalapril group (percent change, −46.7% vs.−25.3%; ratio of change with sacubitril–valsartan vs. enalapril, 0.71; P<0.001) (Figure 1).
- Importantly, greater reduction in the NT-proBNP concentration with sacubitril–valsartan than with enalapril was evident from week 1 (ratio of change, 0.76; 95% CI, 0.69 to 0.85).
- There was no significant difference in terms of rates of worsening renal function, hyperkalemia, symptomatic hypotension, and angioedema between the two groups.
- Treatment discontinuation attributed to adverse events of the medication was also similar in both the study groups.
- Patients in the sacubitril-valsartan group had a 44% relative reduction in the incidence of rehospitalization for HF as compared to those in the enalapril group (8% vs. 13.8%, hazard ratio [HR]; 0.56, 95% CI; 0.30-1.48).
- Patients treated with sacubitril-valsartan also had a 46% relative reduction in the risk of composite serious clinical events (death, rehospitalization for HF, implantation of an LV device, and inclusion on the list of patients eligible for heart transplantation) as compared to those in the enalapril group (9.3% vs. 16.8%, HR; 0.54, 95% CI 0.37-0.79).
Conclusions
- Initiating sacubitril–valsartan therapy among patients hospitalized for acute decompensated HF was associated with a greater reduction in the NT-proBNP concentration as compared to enalapril.
- There was no significant difference between rates of worsening renal function, hyperkalemia, symptomatic hypotension, and angioedema between the two groups.
New Eng J Med. Nov 11, 2018 (Published Online); DOI: 10.1056/NEJMoa1812851.











