

Higher Relative Bioavailability of Calcium from Calcium Orotate than Calcium Carbonate



Introduction
The incidence of osteoporosis in India is significant and rising. Previous studies have reported a reduction in bone mineral density (BMD) by 1-3% per month in pregnant women which is much higher than BMD loss of 1-3% per year in postmenopausal women. Low relative bioavailability and gastrointestinal side effects are associated with the available calcium salts. Calcium orotate is a calcium salt of orotic acid, which ensures target specific delivery of calcium due to its dissociation in the osteoblasts. It has the highest elemental calcium absorption of 95% and is well tolerated. Maximum bone mineralization is ensured as it is the only calcium which directly deposits in the bone. However, there are no studies comparing the bioavailability of calcium orotate with other calcium salts.
Aim
This study compares the relative bioavailability of a single dose calcium orotate with calcium carbonate in healthy Indian adults under fasting conditions.
Method
Study Design
- Open-label, randomized, three-treatment, three-period, balanced, three-sequence, single dose, crossover study
Patient Profile
- Healthy male adults with a mean age of 24.9 years, and body mass index (BMI) of 21.19 kg/m2
- Non-smokers, non-alcoholic consumers, and non-tobacco chewers
Treatment Strategy
- A total of 14 males were randomized to receive either:
- Calcium carbonate containing equimolar amount of elemental calcium and vitamin D3 125 IU
- Test product (T) – Calcium orotate containing equimolar amount of elemental calcium
- Placebo
- All the subjects received one tablet orally after overnight fasting of 10 hours
- A total of 8 blood samples of 5 ml each were collected from each subject
- Pre-dose sample was collected within 1 hr prior to dosing
- The post-dose samples were collected at 0.5, 1, 1.5, 2.25, 3, 3.75 and 4.5 hours after dosing
End Points
- Serum calcium
- Serum intact parathyroid hormone (iPTH)
- Maximum increment in serum calcium concentration ( Cmax)
- Increment in area under curve for serum calcium ( AUC)
Results
- There were no significant differences in the mean baseline predose values for either serum calcium and serum iPTH concentrations
- However, there were significant postdose differences in the treatment groups as seen in Table 1.
|
Time (hrs) |
Serum calcium |
Serum iPTH |
||||
|
|
Calcium orotate (%) |
Calcium carbonate (%) |
Placebo (%) |
Calcium orotate (%) |
Calcium carbonate (%) |
Placebo (%) |
|
0.5 |
4 |
-6 |
1 |
-19 |
-2 |
9 |
|
1 |
19 |
-3 |
0 |
-49 |
-41 |
-8 |
|
1.5 |
19 |
6 |
1 |
-44 |
-40 |
4 |
|
2.25 |
7 |
6 |
-1 |
-48 |
-46 |
8 |
|
3 |
4 |
2 |
1 |
-56 |
-49 |
3 |
|
3.75 |
4 |
2 |
-4 |
-64 |
-47 |
-6 |
|
4.5 |
5 |
3 |
-3 |
-71 |
-41 |
3 |
- The serum calcium levels rose steadily reaching a plateau of 19% above baseline by 1 hr post-dose and remained steady upto 1.5 hrs postdose
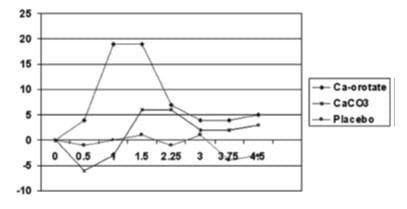
- AUC values were significantly higher in the calcium orotate group as compared to the other 2 groups (p<0.05), indicating better absorption of calcium from calcium orotate as compared to calcium carbonate
- There were significant greater reductions in serum iPTH concentrations after administration of calcium orotate as compared to the 2 groups at 3 hrs postdose and remained persistent throughout the study period
- None of the treatment groups reported incidence of any adverse events
Conclusion
Calcium orotate was associated with -
- Significantly higher oral bioavailability than calcium carbonate
- Rapid, early and higher rate and extent of absorption compared to calcium carbonate
- Substantially and significantly greater increases in serum calcium concentration, greater DAUC for serum calcium increment, and greater decreases in iPTH than equimolar amounts of calcium from supplements based on calcium carbonate.
Obs & Gynae Today 2009,14(10):504-08.












