

Efficacy and Safety of Sacubitril/Valsartan in HFrEF Patients with Low SBP: Insights from PARADIGM-HF



Background
Heart failure (HF) patients with higher systolic blood pressure (SBP) have a worse prognosis as compared to those with lower SBP. Appallingly, such patients with lower SBP are not appropriately treated at times due to concern of further reductions in BP. The fact that sacubitril/valsartan brings about greater reduction in BP as compared to angiotensin converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) alone, is the major concern among physicians while treating their low SBP patients.
Aim
To analyze the efficacy and safety of sacubitril/valsartan vs. enalapril based on the baseline SBP, and as per SBP post-randomization, in the PARADIGM-HF (Prospective Comparison of angiotensin receptor-neprilysin inhibitor [ARNI] with an ACE inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure) trial.
Patient Profile
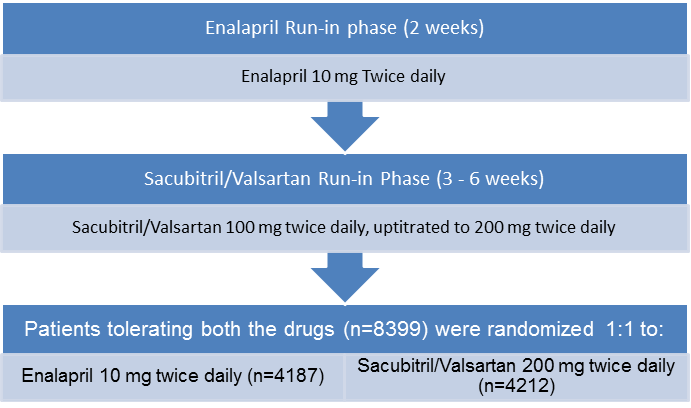
- Patients (age ≥18 years; n=8399) with New York Heart Association (NYHA) class II to IV symptoms having an ejection fraction of ≤40% (changed to ≤35% by protocol amendment) and plasma B-type natriuretic peptide (BNP) ≥150 pg/mL (or N-terminal pro-BNP [NTproBNP] ≥600 pg/mL)
- Patients with lower levels of natriuretic peptides (BNP ≥100 pg/ml or NTproBNP ≥400 pg/ml) were eligible only if they had been hospitalized for HF within 12 months.
- Patients on ongoing therapy were required to tolerate ACE inhibitor or ARB equivalent to at least enalapril 10 mg daily for at least 4 weeks before screening along with stable doses of a ?-blocker (unless contraindicated or not tolerated) and a mineralocorticoid antagonist (if indicated).
- Patients with symptomatic hypotension or an SBP <100mmHg at screening or <95 mmHg at randomization were excluded
Method
Study Design
- Multi-center, randomized, double blind trial with a single blind run-in period
Treatment Strategy
- Reduction in the dose or discontinuation of concomitantly administered BP lowering drugs (e.g. nitrates and diuretics), except guideline-recommended disease-modifying drugs for heart failure (e.g. beta-blockers and mineralocorticoid receptor antagonists) was recommended in case of incident symptomatic hypotension during the study period.
- A strategy of dose reduction or temporary discontinuation of the study drug was also employed in case of hypotension (or other adverse effects).
- Patients were categorized as per baseline SBP as follows:
- <110 mmHg (n=1747)
- 110 to <120 mmHg (n=1931)
- 120 to <130 mmHg (n=2059)
- 130 to <140 mmHg (n=1477)
- ≥140 mmHg (n=1185)
Outcomes
- Change in SBP from baseline (up to 4 months and till end of the follow-up) as per the treatment assignment
- Impact of SBP change on primary outcome (composite of cardiovascular death or heart failure hospitalization)
- Impact of SBP change on secondary outcomes (time to death from any cause and change in the clinical summary score on the Kansas City Cardiomyopathy Questionnaire ([KCCQ])
Result
- An increase in SBP was evident in patients with the lowest baseline SBP, while it decreased in patients with a higher SBP at baseline. This trend was evident in both the groups throughout the follow-up period
- Patients treated with sacubitril/valsartan had lower SBP post-randomization as compared to those treated with enalapril across the SBP range under consideration. Overall, SBP at 4 months was nearly 4-6 mmHg lower in the sacubitril/valsartan group vs. the enalapril group.
- Patients with the lowest SBP had highest all-cause and cardiovascular mortality. A U-shaped relationship was evident between SBP and the rate of HF hospitalization with patients with lower SBP having greater risk of HF hospitalization. The risk of HF hospitalization was also higher amongst the patients with higher SBP (SBP <140 mmHg).
- Sacubitril/valsartan yielded consistent benefits over enalapril across all baseline SBP categories for all outcomes.
- Comparison of results in patients with SBP ≤100 mmHg (low BP) vs. those with SBP >100 mmHg (high BP) at baseline indicated that amongst low SBP group, sacubitril/valsartan treatment was associated with distinctly lower mortality as well as morbidity vs. enalapril. The sacubitril/valsartan vs. enalapril hazard ratio for the primary endpoint was 0.88 in group with baseline SBP <110 mmHg and 0.81 for those with a SBP ≥140mmHg (P for interaction = 0.55).
- A fall of five or more units in the KCCQ clinical summary score (an indicator of significant clinical worsening) occurred in fewer patients in the sacubitril/valsartan group as compared to the enalapril arm.
- Patients with baseline SBP <110 mmHg had more frequent episodes of symptomatic hypotension (SBP<90 mmHg), irrespective of allocated treatment.
Conclusions
- Although lower SBP was associated with worse outcomes, amongst patients who tolerated sacubitril/valsartan, this treatment was beneficial over enalapril across the entire SBP range in the PARADIGM-HF trial when patients were taking other guideline recommended medications.
- As compared to patients with higher SBP, those with lower SBP may obtain greater absolute benefits with sacubitril/valsartan treatment, though; the incidence of hypotension-related side effects may be greater.
Eur Heart J. 2017; 38, 1132–43












