

Efficacy and Safety of Remdesivir 5 Days Course verses 10 Days Course in Treatment of Patients with Severe Covid-19 Disease



Introduction
Remdesivir is a prodrug of an adenosine analogue with demonstrated antiviral activity against a broad range of RNA virus families. It has shown nanomolar invitro activity against SARS-CoV-2 in human airway epithelial cells and clinical and virologic efficacy in a primate model of SARS-CoV-2.
Aim
To evaluate the efficacy and safety of treatment with remdesivir for 5 or 10 days in patients with severe Covid-19 disease
Patient Profile
- Hospitalized patients who were at least 12 years of age who had SARS-CoV-2 infection confirmed by polymerase-chain-reaction as say within 4 days before randomization.
- Eligible patients had radiographic evidence of pulmonary infiltrates and either had an oxygen saturation of 94% or less while they were breathing ambient air or were receiving supplemental oxygen
Methods
- An ongoing phase 3 trial,open-label, randomized, multicenter trial
- Conducted at 55 hospitals in the United States, Italy, Spain, Germany, Hong Kong, Singapore, South Korea, and Taiwan between March 6 and March 26, 2020
Study Design
Study Drug
All the patients received 200 mg of remdesivir on day 1, followed by 100 mg of remdesivir once daily for the subsequent 4 or 9 days
Endpoints
- Primary Endpoints
- Clinical status assessed on day 14 on a 7-point ordinal scale consisting of the following categories: 1, death 2, hospitalized, receiving invasive mechanical ventilation or ECMO; 3, hospitalized, receiving noninvasive ventilation or high-flow oxygen devices; 4, hospitalized, requiring low-flow supplemental oxygen; 5, hospitalized, not requiring supplemental oxygen but receiving ongoing medical care (related or not related to Covid-19); 6, hospitalized, requiring neither supplemental oxygen nor ongoing medical care (other than that specified in the protocol for remdesivir administration); and 7, not hospitalized
- Secondary Endpoints
- The proportion of patients with adverse events that occurred on or after the first dose of remdesivir for up to 30 days after the last dose
- Prespecified exploratory endpoints included the
- Time to clinical improvement (defined as an improvement of at least 2 points from baseline on the 7-point ordinal scale)
- Time to recovery (defined by the National Institute of Allergy and Infectious Diseases [NIAID] as an improvement from a baseline score of 2 to 5 to a score of 6 or 7)
- Time to modified recovery (defined as an improvement from a baseline score of 2 to 4 to a score of 5 to 7 or from a score of 5 to a score of 6 or 7), and death from any cause
Results
Table 1: Baseline Characteristics
|
Characteristic |
5-Day Group (N = 200) |
10-Day Group (N = 197) |
|
Median age (IQR) — yr |
61 (50–69) |
62 (50–71) |
|
Male sex — no. (%) |
120 (60) |
133 (68) |
|
Race — no./total no. (%)† |
|
|
|
White |
142/200 (71) |
134/192 (70) |
|
Black |
21/200 (10) |
23/192 (12) |
|
Asian |
20/200 (10) |
25/192 (13) |
|
Other |
17/200 (8) |
10/192 (5) |
|
Median body-mass index (IQR)‡ |
29 (25–34) |
29(25–33) |
|
Coexisting conditions of interest — no. (%) |
|
|
|
Diabetes |
47 (24) |
43 (22) |
|
Hyperlipidemia |
40 (20) |
49 (25) |
|
Hypertension |
100 (50) |
98 (50) |
|
Asthma |
27 (14) |
22 (11) |
|
Clinical status on the 7-point ordinal scale — no. (%)§ |
|
|
|
2: Receiving invasive mechanical ventilation or ECMO |
4 (2) |
9 (5) |
|
3: Receiving noninvasive ventilation or high-flow oxygen |
49 (24) |
60 (30) |
|
4: Receiving low-flow supplemental oxygen |
113 (56) |
107(54) |
|
5: Not receiving supplemental oxygen but requiring medical care |
34 (17) |
21 (11) |
|
Median duration of hospitalization before first dose of remdesivir |
2 (1–3) |
2 (1–3) |
|
(IQR) — days |
|
|
|
Median duration of symptoms before first dose of remdesivir (IQR) |
8 (5–11) |
9 (6–12) |
|
— days |
|
|
|
Median AST level (IQR) — U/liter¶ |
41 (29–58) |
46 (34–67) |
|
Median ALT level (IQR) — U/liter |
32 (22–50) |
36 (23–58) |
|
Median creatinine clearance by Cockcroft–Gault (IQR) — ml/min |
106 (80-142) |
103 (80–140) |
* Percentages may not total 100 because of rounding. ALT denotes alanine aminotransferase, AST aspartate aminotransferase, and IQR interquartile range.
† Race was reported by the patients.
‡ The body-mass index is the weight in kilograms divided by the square of the height in meters.
§ P = 0.02 for the comparison between the 5-day group and the 10-day group by the Wilcoxon rank-sum test.
¶ P = 0.008 for the comparison between the 5-day group and the 10-day group by the Wilcoxon rank-sum test.
- High-flow oxygen support was required at baseline by more patients in the 10-day group than in the 5-day group (30% vs 24%)
- As a result, patients in the 10-day group had significantly worse clinical status than those in the 5-day group (P = 0.02)
- 172 (86%) in 5 -day group and 197 patients in the 10-day group, 86 (44%), completed the treatment course for a median duration of 5 days and 9 days respectively
Efficacy
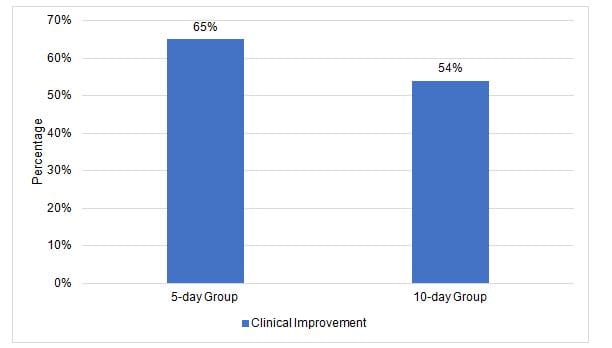
- No significant difference was observed in efficacy between 5-day and 10-day courses of remdesivir
|
Characteristic |
5-Day Group (N=200) |
10-Day Group (N=197) |
Baseline-Adjusted Difference* P = 0.14† |
|
|
|
|
|
|
Clinical status at day 14 on the 7-point ordinal scale — no. of patients (%) |
|
|
|
|
1:Death |
16 (8) |
21 (11) |
|
|
2: Hospitalized, receiving invasive mechanical ventilation or ECMO |
16 (8) |
33 (17) |
|
|
3: Hospitalized, receiving noninvasive ventilation or high-flow oxygen |
9 (4) |
10 (5) |
|
|
4: Hospitalized, requiring low-flow supplemental oxygen |
19 (10) |
14 (7) |
|
|
5: Hospitalized, not receiving supplemental oxygen but requiring ongoing medical care |
11 (6) |
13 (7) |
|
|
6: Hospitalized, not requiring supplemental oxygen or ongoing medical care |
9 (4) |
3 (2) |
|
|
7. Not hospitalized |
120 (60) |
103 (52) |
|
|
Time to clinical improvement (median day of 50% cumulative incidence‡) |
10 |
11 |
0.79 |
|
Clinical improvement — no. of patients (%) |
|
|
|
|
Day 5 |
33 (16) |
29 (15) |
0.2% |
|
Day 7 |
71 (36) |
54 (27) |
−5.0%
|
|
Day 11 |
116 (58) |
97 (49) |
−4.8%
|
|
Day 14 |
129 (64) |
107 (54) |
−6.5%
|
|
Time to recovery (median day of 50% cumulative incidence‡) |
10 |
11 |
0.81
|
|
Recovery — no. of patients (%) |
|
|
|
|
Day 5 |
32 (16) |
27 (14) |
0.1%
|
|
Day 7 |
71 (36) |
51 (26) |
−6.0%
|
|
Day 11 |
115 (58) |
97 (49) |
−3.7%
|
|
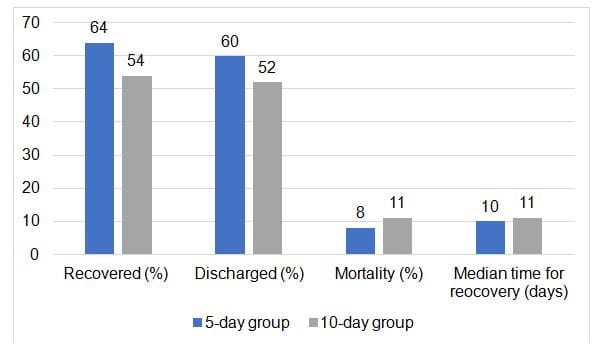
Day 14 |
129 (64) |
106 (54) |
−6.3%
|
|
Time to modified recovery (median day of 50% cumulative incidence‡) |
9 |
10 |
0.82
|
|
Modified recovery — no. of patients (%) |
|
|
|
|
Day 5 |
51 (26) |
41 (21) |
−2.3% |
|
Day 7 |
84 (42) |
69 (35) |
−3.4% |
|
Day 11 |
128 (64) |
106 (54) |
−5.7% |
|
Day 14 |
140 (70) |
116 (59) |
−6.7% |
* Differences are expressed as rate differences, except in the case of time to clinical improvement, time to recovery, and time to modified recovery, for which differences are expressed as hazard ratios; for these time-to-event endpoints, the hazard ratio and its 95% confidence interval were estimated from a cause-specific proportional-hazards model including treatment and baseline clinical status as covariates. For events at prespecified time points (e.g., days 5, 7, 11, and 14), the difference in the proportion of subjects with an event under evaluation between treatment groups and the 95% confidence interval were estimated from the Mantel–Haenszel proportions adjusted according to baseline clinical status.
† The P-value was calculated from a Wilcoxon rank-sum test stratified by baseline clinical status.
‡ Clinical improvement was defined as an improvement of at least 2 points from baseline on the 7-point ordinal scale; recovery was defined as an improvement from a baseline score of 2 to 5 to a score of 6 or 7, and modified recovery was defined as an improvement from a baseline score of 2 to 4 to a score of 5 to 7 or from a score of 5 to a score of 6 or 7. Cumulative incidence functions were calculated for each treatment group for days to the event under evaluation (i.e., clinical improvement, recovery, or modified recovery), with death as the competing risk. Data for patients not achieving the event under evaluation at the last assessment were censored on the day of the last clinical assessment. Patients who died before achieving the event under evaluation were considered to have experienced a competing event.
- In the overall population, discharge rates were higher among patients who had had symptoms for less than 10 days before receiving the first dose of remdesivir (62%) than among those who had had symptoms for 10 or more days before receiving the first dose (49%).
- Effect of an additional 5 days of treatment with remdesivir
- Among patients receiving mechanical ventilation or ECMO at day 5, 40% (10 of 25) in the 5-day group had died by day 14, as compared with 17% (7 of 41) in the 10-day group
- Treatment with remdesivir beyond 5 days among patients who were receiving noninvasive positive-pressure ventilation or high-flow oxygen, receiving low-flow oxygen, or breathing ambient air did not appear to improve outcomes.
Safety
- Adverse events experienced by patients were similar in the two groups
- 5-day group: 70%
- 10-day group: 74%
- The most common adverse events overall were
- nausea (10% in the 5-day group vs 9% in the 10-day group)
- acute respiratory failure (6% vs 11%),
- increased ALT (6% vs. 8%)
- constipation (7% in both groups)
|
Event or Abnormality |
5-Day Group (N = 200) |
10-Day Group (N = 197) |
|
Any adverse event — no. of patients (%) |
141 (70) |
145 (74) |
|
Nausea |
20 (10) |
17 (9) |
|
Acute respiratory failure |
12 (6) |
21 (11) |
|
Alanine aminotransferase increased |
11 (6) |
15 (8) |
|
Constipation |
13 (6) |
13 (7) |
|
Aspartate aminotransferase increased |
10 (5) |
13 (7) |
|
Hypokalemia |
10 (5) |
12 (6) |
|
Hypotension |
9 (4) |
12 (6) |
|
Respiratory failure |
7 (4) |
14 (7) |
|
Insomnia |
10 (5) |
11 (6) |
|
Acute kidney injury |
4 (2) |
15 (8) |
|
Adverse event leading to discontinuation of treatment — no. of patients (%) |
9 (4) |
20 (10) |
|
Any serious adverse event |
42 (21) |
68 (35) |
|
Acute respiratory failure |
10 (5) |
18 (9) |
|
Respiratory failure |
5 (2) |
10 (5) |
|
Septic shock |
2 (1) |
5 (3) |
|
Acute respiratory distress syndrome |
1 (<1) |
5 (3) |
|
Hypoxia |
2 (1) |
4 (2) |
|
Respiratory distress |
3 (2) |
4 (2) |
|
Dyspnea |
4 (2) |
1 (1) |
|
Pneumothorax |
2 (1) |
3 (2) |
|
Viral pneumonia |
3 (2) |
2 (1) |
|
Aminotransferase levels increased |
3 (2) |
2 (1) |
|
Any grade ≥3 laboratory abnormality — no. of patients/total no. (%) |
53/195 (27) |
64/191 (34) |
|
Selected grade ≥3 laboratory abnormalities — no. of patients/total no. (%) |
|
|
|
Creatinine clearance decreased |
|
|
|
Grade 3 |
13/193 (7) |
13/188 (7) |
|
Grade 4 |
5/193 (3) |
23/198 (12) |
|
ALT elevation |
|
|
|
Grade 3 |
8/194 (4) |
11/191 (6) |
|
Grade 4 |
4/194 (2) |
5/191 (3) |
|
AST elevation |
|
|
|
Grade 3 |
11/194 (6) |
7/190 (4) |
|
Grade 4 |
3/194 (2) |
4/190 (2) |
|
Bilirubin increased |
|
|
|
Grade 3 |
1/193 (1) |
3/190 (2) |
|
Grade 4 |
0 |
1/190 (1) |
* Adverse events listed are those that occurred in at least 5% of patients in either treatment group, and serious adverse events listed are those that occurred in 5 or more patients.
Conclusion
- The study demonstrated no significant difference in efficacy between a 5-day course and a 10-day course of intravenous remdesivir treatment in patients with severe Covid-19 due to SARS-CoV-2 who did not require mechanical ventilation at baseline
- Patients who progress to mechanical ventilation may benefit from 10 days of remdesivir treatment
Reference
N Engl J Med. 2020 May 27. doi: 10.1056/NEJMoa2015301.











