

Reduction in CV mortality and ischemic events in patients with acute coronary syndromes: Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) trial
CURE (Clopidogrel in Unstable Angina to Prevent Recurrent Events)

18 Mar, 14


CURE
CURE (Clopidogrel in Unstable Angina to Prevent Recurrent Events)
Aim
To compare the efficacy and safety of the early and long-term use of clopidogrel plus aspirin with those of aspirin alone in patients with acute coronary syndromes (ACS)
Study Patients
ACS (N = 12,562)
Study Drugs
Clopidogrel (300 mg followed by 75 mg) + Aspirin (75-325 mg) vs Placebo + Aspirin
Study Duration
3-12 months (mean 9 months)
Results
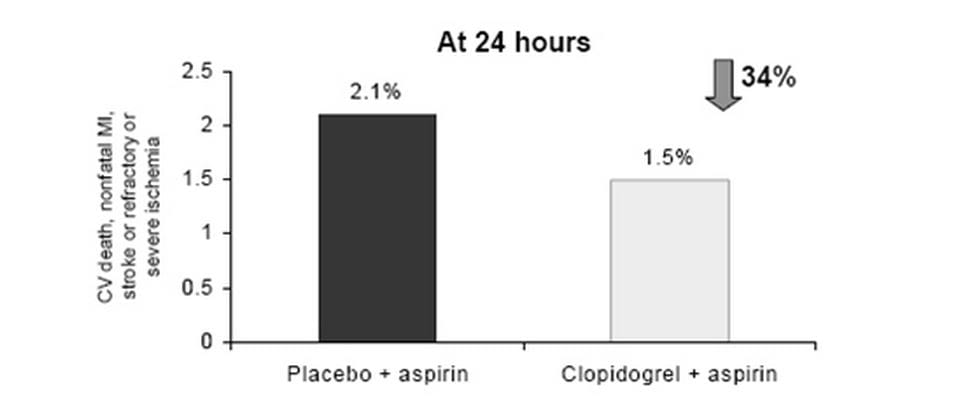
- Reductions in events were seen as early as within 24 hours.
- Benefits observed as early as 30 days and sustained at the end of 1 year
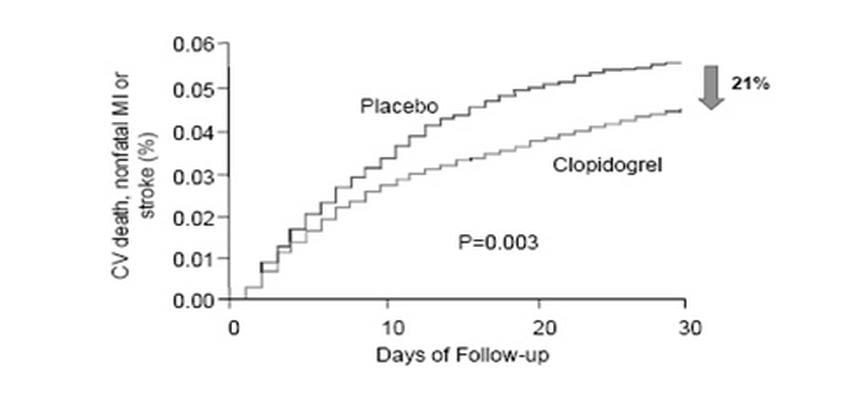
- The addition of clopidogrel reduced the risk of cardiovascular death, nonfatal myocardial infarction or stroke by 20%.
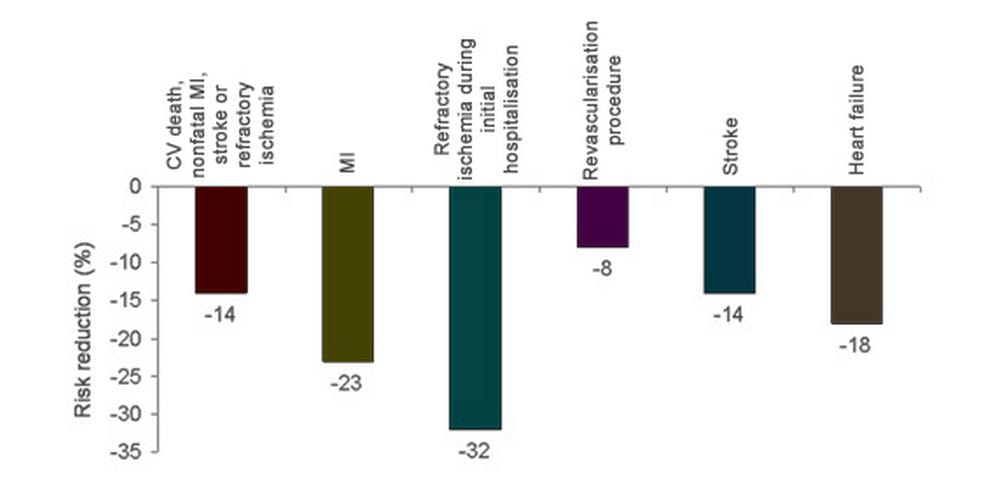
- Risk of cardiovascular death, nonfatal myocardial infarction, stroke or refractory ischemia was reduced by 14%.
- Risk of myocardial infarction was reduced by 23% while risk of stroke was reduced by 14%.
- Risk of heart failure was reduced by 18%.
- Need for revascularisation procedures was reduced by 8% and risk of refractory ischemia during initial hospitalisation was reduced by 32%.
- Importantly, the need for thrombolytics and GP IIb/IIIa antagonists was also reduced.
Safety
- Bleeding more common in clopidogrel + aspirin group compared to aspirin alone (3.7% vs 2.7%)
- No increased risk of fatal bleeding or hemorrhagic stroke
- Risk of neutropenia and thrombocytopenia similar
- Discontinuation rates similar
Conclusion
Early addition of clopidogrel to existing aspirin therapy provides additional benefits as compared to aspirin alone in ACS patients. These benefits were maintained for long-term.
NEJM 2001; 345: 494-502

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


