A substantial proportion of patients receiving fibrinolytic therapy for myocardial infarction with ST-segment elevation have inadequate reperfusion or reocclusion of the infarct-related artery, leading to an increased risk of complications and death.
Prior clopidogrel studies such as CREDO and CURE have been conducted in patients with non-ST elevation acute coronary syndromes.
However, benefits of addition of clopidogrel in patients of MI with ST-segment elevation and receiving fibrinolytic therapy, including aspirin, has not been evaluated.
To evaluate whether the addition of clopidogrel to standard fibrinolytic therapy, including aspirin, would improve infarct-related artery patency and decrease ischemic complications in patients with ST-segment elevation MI (STEMI).
Multicenter, randomized, double-blind, placebo controlled study.
3491 patients, aged 18-75 years, presenting with ischemic discomfort at rest within 12 hours before randomization and which lasted more than 20 minutes; ST-segment elevation of at least 0.1 mV in at least two contiguous limb leads, ST-segment elevation of at least 0.2 mV in at least two contiguous precordial leads, or left bundle-branch block that was not known to be old; and if they were scheduled to receive a fibrinolytic agent, an anticoagulant (if a fibrin-specific lytic agent was prescribed) and aspirin.
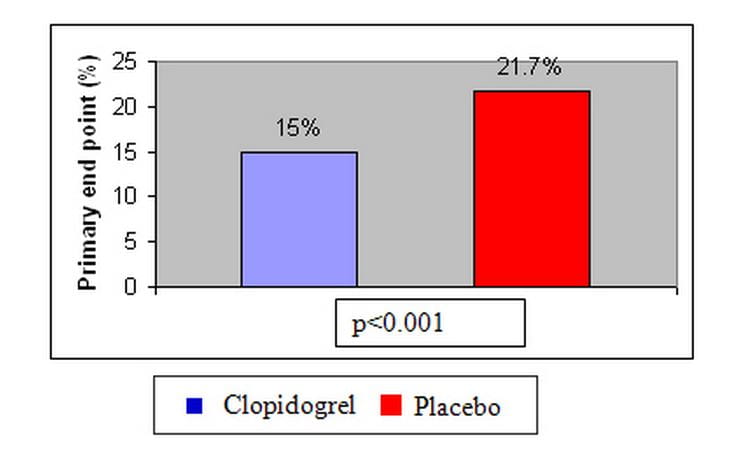
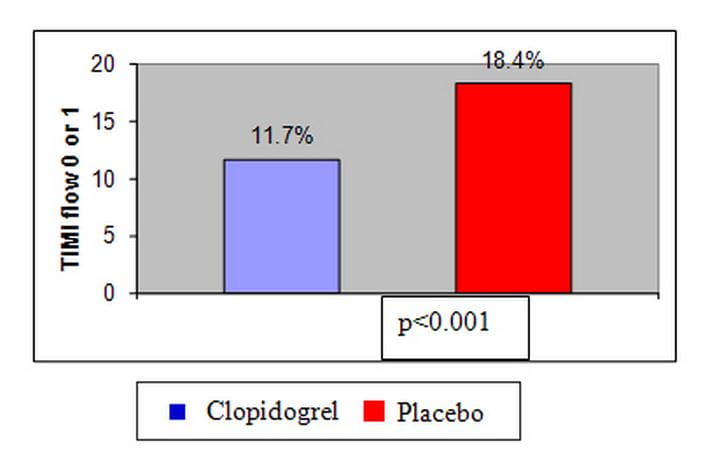
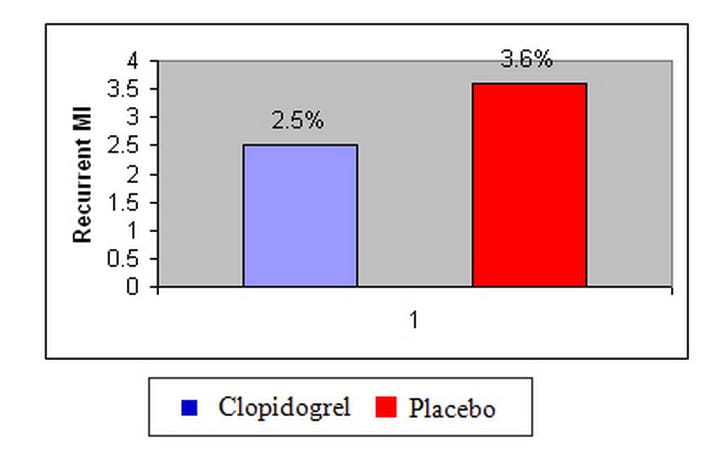
Composite of death or recurrent MI or an occluded infarct-related artery (TIMI flow 0 or 1) on angiography.
Addition of clopidogrel to aspirin and a standard fibrinolytic regimen improves the patency rate of the infarct-related artery and reduces ischemic complications in STEMI patients aged 75 years or younger.