

Cardioprotective Effect of Oral Bisphosphonates



Introduction
Osteoporosis or low bone mass does not exist in isolation, but often co-exists with other chronic diseases, particularly cardiovascular [CV]. Awareness of the need for management of CV risk factors alongside fracture risk is growing, given multiple reports of increased CV mortality following osteoporotic fragility fracture.
Aim
To determine the risk of incident CV disease associated with oral bisphosphonate (oBP) use in oral BP (oBP) users and non-users
Patient Profile
- Individuals aged ≥45 years referred for bone mineral density (BMD) testing
- Individuals were considered exposed (oBP user) if they filled at least one prescription for an oBP (representing new users) from 1 January 2003 to 31 December 2014 had a real BMD (hip and spine) determined by DXA within two years of the prescription
Methods
- Cohort study
- 5,643 oBP users (4564 women; 80.9%) and 21,879 non-users (16730 women; 76.5%) with clinical indication for BMD assessment
- Alendronate accounted for 96% of oBP prescriptions were included in analysis
Study Outcomes
- Hospitalization for any CV event
- Secondary study outcomes were specific CV events. Negative (inguinal hernia surgery and ingrown toenail) and positive (fragility fracture) control outcomes assessed systemic bias
Results
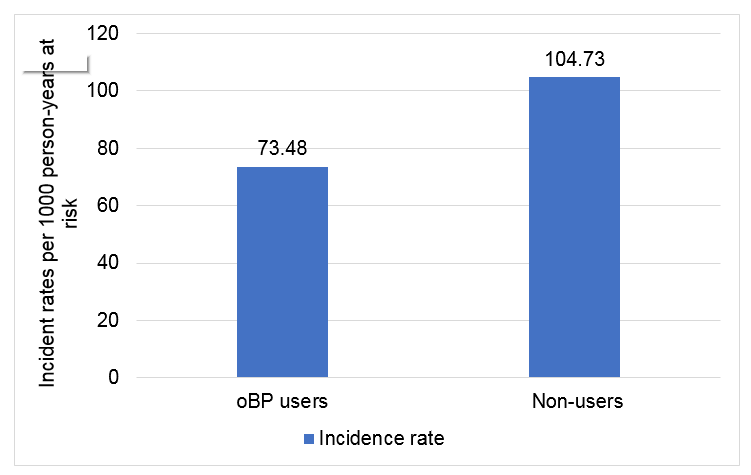
- For the primary outcome, there were 406 (15.8%) events in oBP users [rate = 73.48 (66.67 to 80.98)] and 837 (18.3%) in non-users [rate=104.73 (97.87 to 112.07)]
- oBP use was associated with a 26% reduced risk of CV events
- oBP use was only associated reduced risk of CV or all-cause mortality
|
Analysis |
Intention-to-treat |
Per-protocol |
|||||
|
Adjustments |
oBP |
oBP & Pscore |
oBP & Pscore & Unbalanced covariates |
oBP |
oBP & Pscore |
oBP & Pscore & Unbalanced covariates |
|
|
Hospitalisation outcomes |
|
|
|
|
|
|
|
|
Any CVD event |
0.74 |
0.68 |
0.67 |
0.90 |
0.84 |
0.82 |
|
|
Atrial fibrillation |
0.67 |
0.60 |
0.63 |
0.79 |
0.71 |
0.74 |
|
|
Cardiac arrhythmia |
0.61 |
0.61 |
0.66 |
0.80 |
0.80] |
0.89 |
|
|
Myocardial infarction |
0.92 |
0.86 |
0.90 |
1.04 |
0.98 |
1.03 |
|
|
Heart failure |
0.76 |
0.68 |
0.65 |
0.97 |
0.90 |
0.84 |
|
|
Stroke |
0.60 |
0.56 |
0.46 |
0.82 |
0.76 |
0.61 |
|
|
Ischaemic stroke |
0.64 |
0.60 |
0.50 |
0.86 |
0.81 |
0.66 |
|
|
Atherosclerotic |
0.45 |
0.42 |
0.35 |
0.63 |
0.59 |
0.51 |
|
|
Aneurysm |
0.55 |
0.53 |
0.57 |
0.72 |
0.69 |
0.75 |
|
|
Peripheral artery disease |
0.73 |
0.71 |
0.65 |
0.95 |
0.92 |
0.88 |
|
|
Mortality outcomes |
|
|
|
|
|
|
|
|
Any CVD death |
0.55 |
0.48 |
0.50 |
0.44 |
0.36 |
0.37 |
|
|
Stroke death |
0.45 |
0.37 |
0.37 |
0.39 |
0.33 |
0.45 |
|
|
Myocardial infarction |
0.64 |
0.56 |
0.53 |
0.67 |
0.52 |
0.47 |
|
|
All-cause |
0.59 |
0.45 |
0.35 |
0.38 |
0.28 |
0.23 |
|
Unbalanced covariates: lumbar spine BMD, osteoporosis in the spine, prior fracture at any site. Pscore = propensity score
Effect of oBP use on Osteoporotic Fractures
- There were 247 (9.6%) fractures in oBP users and 630 (13.8%) fractures in propensity score-matched non- users with an adjusted HR of 0.26
- Oral BP use was associated with an anticipated reduction in fracture rate, but was not associated with inguinal hernia repair or ingrown toenails
Conclusion
- There was a reduced risk of CV events in the cohort of Danish oral BP users matched on a clinical indication for DXA to non-users
- The data supports findings from BP RCTs showing a reduction in CV events
- Additional adjustment for BMD did not alter outcomes, which questions the prognostic value of BMD on CV risk in the setting of osteoporosis
Reference
J Clin Endocrinol Metab.2020 ;105(10):dgaa481












