

CANVAS Program: Canagliflozin Delays the Initiation of Insulin or other Antihyperglycemic Agents in T2DM Patients



Introduction
The “CANagliflozin cardioVascular Assessment Study” (CANVAS) Program has already demonstrated the cardiovascular (CV) benefits of canagliflozin in patients with type-2 diabetes mellitus (T2DM) and established cardiovascular disease (CVD) or high CV risk. During the course of CANVAS program a higher proportion of patients treated with placebo rather than canagliflozin initiated new antihyperglycemic agents (AHA). Nevertheless, the timing of initiating specific classes of AHAs has not been reported.
Aim
To compare initiation of insulin and other AHAs with canagliflozin vs. placebo in participants of CANVAS Program and to quantify the extent to which canagliflozin spares the need for initiation of insulin.
Patient Profile
- Patients with T2DM [glycated hemoglobin (HbA1c) between ≥7% and ≤10.5%, age ≥ 30 years, n=10142)
- The study participants either had a history of symptomatic atherosclerotic CVD or were aged ≥50 years with ≥2 CV risk factors
Methods
Study Design
- Post hoc analysis of the CANVAS Program
- The CANVAS Program comprised of 2 double-blind, randomized, placebo-controlled trials (CANVAS and CANVAS-R)
Treatment Strategy
- Patients were randomized to receive canagliflozin or placebo along with other background antidiabetic medications.
Outcomes
- New initiation of AHAs [defined as post randomisation initiation of any AHA not taken at baseline: insulin, metformin, dipeptidyl peptidase-4 (DPP-4) inhibitor, glucagon-like peptide-1 receptor agonist (GLP-1RA) and sulphonylurea]
Follow-up
- Median follow-up 3.6 years
Results
- Baseline characteristics and AHA use were similar in patients treated with canagliflozin and placebo. At baseline, nearly 77% of the study subjects were on metformin, 50% on insulin, 43% on sulphonylurea, 12% on a DPP-4 inhibitor and 4% on a GLP-1 RA.
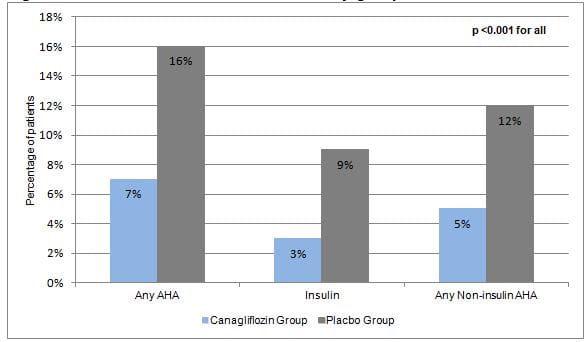
- After 1 year significantly fewer patients treated with canagliflozin vs. placebo initiated any AHA, insulin or any non-insulin AHA (Figure 1). Although the overall AHA initiation rates increased over time, they were consistently lower with canagliflozin vs. placebo during the entire study period.
- The time difference for patients in the canagliflozin and placebo groups being initiated on insulin from the beginning of the trial was about two years (160 weeks vs. 52 weeks). The likelihood of initiating insulin during the study was 2.7 times lower for patients treated with canagliflozin vs. placebo [Hazard ratio (HR), 0.37; 95% CI: 0.31-0.43; p<0.001]
- The likelihood of initiating any AHA (HR, 0.47 [95% CI: 0.43, 0.51]), or any non-insulin AHA (HR, 0.50 [95% CI: 0.45, 0.55]) was also significantly lower with canagliflozin vs. placebo (all p <0.001)
- Time to initiation of other AHAs, including metformin, DPP-4 inhibitors, GLP-1 RA and sulphonylureas, was also significantly delayed in canagliflozin-treated vs. placebo-treated patients (p<0.001 for each).
Conclusion
- Amongst CANVAS participants, canagliflozin was associated with a lesser likelihood of initiating insulin or new AHA.
Diabetes Obes Metab. Jul 20, 2020 (Published Ahead of Print); doi: 10.1111/dom.14143.












