

Azilsartan is More Effective than Olmesartan in Reducing BP in Hypertensive Patients

13 Apr, 17


Aim
To assess the anti-hypertensive efficacy and safety of the latest angiotensin II receptor blocker (ARB), azilsartan medoxomil, compared to placebo and another ARB, olmesartan medoxomil
Patient Profile
- 1275 patients with primary hypertension [defined as sitting through clinic systolic blood pressure (SBP) ≥150 mm Hg and ≤ 180 mm Hg and 24-hour mean SBP ≥130 mm Hg and ≤ 170 mm Hg]
Method
Study Design
- Randomized, multicenter, parallel-group, double-blind, placebo-controlled trial
Treatment Strategy
- Patients were randomized to receive either placebo, azilsartan medoxomil 20/ 40/ 80 mg/day or olmesartan medoxomil 40 mg/day
Duration
- 6 weeks
Key Primary End Point
- Change in 24-hour mean SBP assessed by ambulatory blood pressure monitoring (ABPM)
Key Secondary End Point
- Change in trough sitting clinic SBP
Other Secondary End Points
- Change from baseline in trough sitting clinic diastolic BP (DBP) by ABPM and proportion of responders (patients who had a reduction in clinic SBP to <140 mm Hg and/or a reduction of ≥ 20 mm Hg)
Results
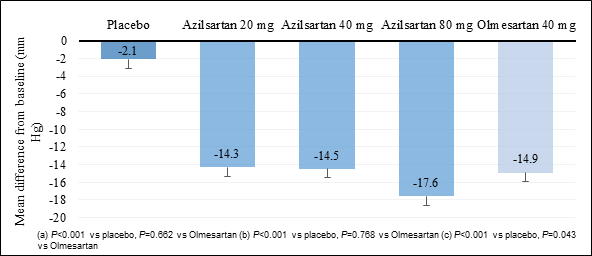
- Both azilsartan medoxomil and olmesartan medoxomil reduced 24-hour mean SBP and clinic SBP, but 80 mg azilsartan offered significantly greater reduction as compared to 40 mg of olmesartan (Figure 1 & 2)
Fig. 1: Reduction in 24-hour mean SBP
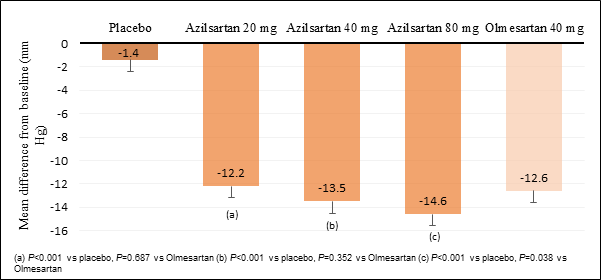
Fig. 2: Reduction in clinic SBP
- Similarly, reduction in clinic DBP was significantly greater with the 80-mg dose of azilsartan medoxomil compared with olmesartan medoxomil 40 mg, with a treatment difference of -1.5 mm Hg (P=0.044)
- The proportion of responders were 48%, 50%, and 57% with azilsartan medoxomil 20 mg, 40 mg, and 80 mg, respectively, as compared to 53% with olmesartan medoxomil 40 mg
- Azilsartan was overall well-tolerated, with adverse event profile of both ARBs being similar to placebo.
Conclusion
- Azilsartan medoxomil was more effective and well tolerated at its maximal dose than the highest dose of olmesartan medoxomil.
J Clin Hypertens (Greenwich). 2011; 13: 81–8.

More From Area Of Interest
You may also like

13 May, 26

17 Apr, 26
Our Research
23 Feb, 26

23 Feb, 26

11 Feb, 26

11 Feb, 26

11 Feb, 26
Latest Items
Journal Scans
26 Jun, 26

26 Jun, 26

26 Jun, 26

25 Jun, 26


