

Azilsartan Effectively Suppresses Morning BP Surge in Hypertensive Patients



Background
Morning blood pressure (BP) surge is a reported risk factor for cardiovascular events and end-organ damage, independent of the 24-hour BP level. Controlling morning BP surge is therefore important to help prevent onset of cardiovascular disease.
Aim
To evaluate the efficacy of azilsartan compared to candesartan in controlling morning BP surge in hypertensive patients with or without baseline BP surges
Patient Profile
Surge Group
- Patients who experienced a morning BP surge [defined as presence of sleep trough surge (i.e. early morning systolic BP minus the lowest night-time systolic BP) of at least 35 mm Hg] at baseline (n=147)
Non-Surge Group
- Patients who did not experience a morning BP surge at baseline (n=401)
Method
Study Design
Randomized, double-blind study (an exploratory analysis)
Study Drugs
- Azilsartan 20 mg daily for the first 8 weeks, followed by 40 mg daily (Surge group: 76; Non-surge group: 197)
- Candesartan cilexetil (candesartan) 8 mg daily for the first 8 weeks, followed by 12 mg daily (Surge group: 71; Non-surge group: 204)
Duration
14 weeks
Efficacy Parameters
- Change in ambulatory BP monitoring (ABPM) parameters: 24-hour mean BP, day-time mean BP, night-time mean BP, lowest night-time BP (mean systolic BP measured during the period 35 min before and after measurement of the lowest sleep systolic BP), early morning BP (mean systolic BP measured during the 2-hour period after awakening), BP before awakening (mean systolic BP measured during the 2-hour period before awakening)
- Change in the sleep through surge and pre-waking surge (i.e. early morning systolic BP minus systolic BP before awakening)
Results
- Overall, ABPM parameters were reduced by both azilsartan and candesartan (Table 1).
- Surge group: Administration of azilsartan decreased the 24-hour mean systolic BP, mean day-time systolic BP, night-time systolic BP, lowest night-time systolic BP, the early morning systolic BP, and the systolic BP before awakening to a significantly greater extent than candesartan
- Non-surge group: Reduction in 24-hour mean systolic BP and mean day-time systolic BP was significantly greater with azilsartan than candesartan. However, reductions in other ABPM parameters were similar in both groups.
|
ABPM parameters |
Groups |
Magnitude of change |
P value (azilsartan vs candesartan) | |
|
Azilsartan |
Candesartan | |||
|
24-hour mean BP (mm Hg) |
Surge |
-15.1 |
-10.0 |
0.0103 |
|
Nonsurge |
-12.2 |
-9.1 |
0.0114 | |
|
Day-time mean BP (mm Hg) |
Surge |
-16.1 |
-9.9 |
0.0071 |
|
Nonsurge |
-10.6 |
-6.8 |
0.0038 | |
|
Night-time mean BP (mm Hg) |
Surge |
-14.0 |
-10.3 |
0.0407 |
|
Nonsurge |
-15.8 |
-13.3 |
0.0951 | |
|
Lowest night-time BP (mm Hg) |
Surge |
-11.9 |
-6.7 |
0.0236 |
|
Nonsurge |
-17.0 |
-15.2 |
0.3618 | |
|
Early morning mean BP (mm Hg) |
Surge |
-21.3 |
-11.1 |
0.0002 |
|
Nonsurge |
-8.7 |
-6.1 |
0.2106 | |
|
BP before awakening (mm Hg) |
Surge |
-15.6 |
-11.2 |
0.0451 |
|
Nonsurge |
-13.6 |
-12.8 |
0.6248 | |
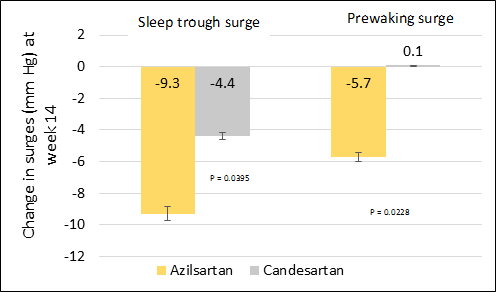
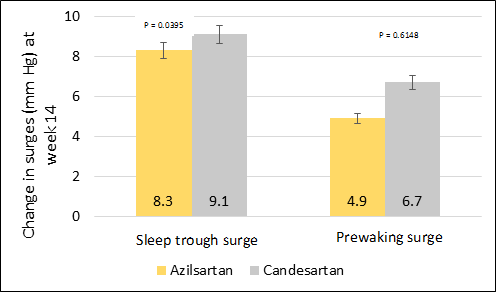
- Both sleep trough surge and the pre-waking surge were significantly reduced by azilsartan in comparison with candesartan in the surge group (Figure 1). This may be attributed to the marked reduction in early morning systolic BP observed with azilsartan.
(a) Surge group
(b) Non- surge group
Conclusion
- Azilsartan exerts a more pronounced effect in suppressing morning BP surge than candesartan. Thus, azilsartan might effectively reduce the risk of future cardiovascular events.
Blood Press Monit. 2014; 19: 164-9












